
Presentation
Rapidly progressive right eye proptosis, chemosis, and visual loss.
Patient Data
ASNR 2016: This case was submitted as part of the American Society of Neuroradiology (ASNR 2016) Case Of The Day competition, in collaboration with Radiopaedia.org.
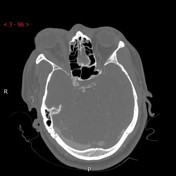

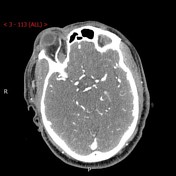
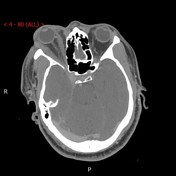

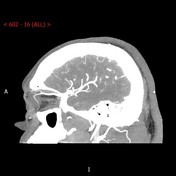
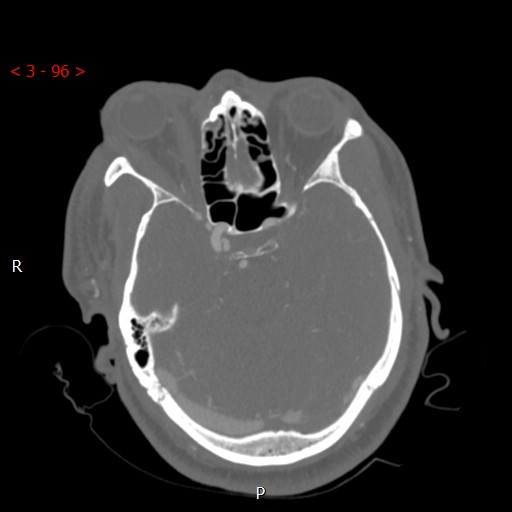
There is asymmetric enlargement of the right superior ophthalmic vein and right cavernous sinus. Enhancing foci are seen in the right cavernous sinus in the arterial phase. Reflux of contrast into the right superior ophthalmic vein is noted with enhancement in the arterial phase. There is right-sided proptosis, diffuse thickening of right extra-ocular muscles, mild periorbital swelling and mild soft tissue stranding/edema in the right intraorbital fat.
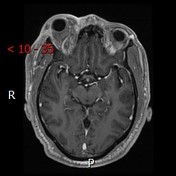

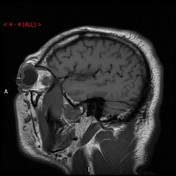
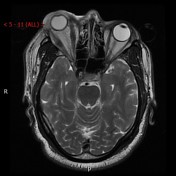
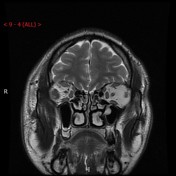

There is right-sided proptosis, stranding/edema in the right intraorbital fat and periorbital soft tissue, diffuse enlargement of the right extraocular muscles and asymmetric enlargement of the right superior ophthalmic vein.
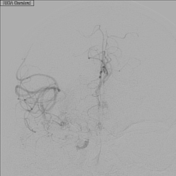



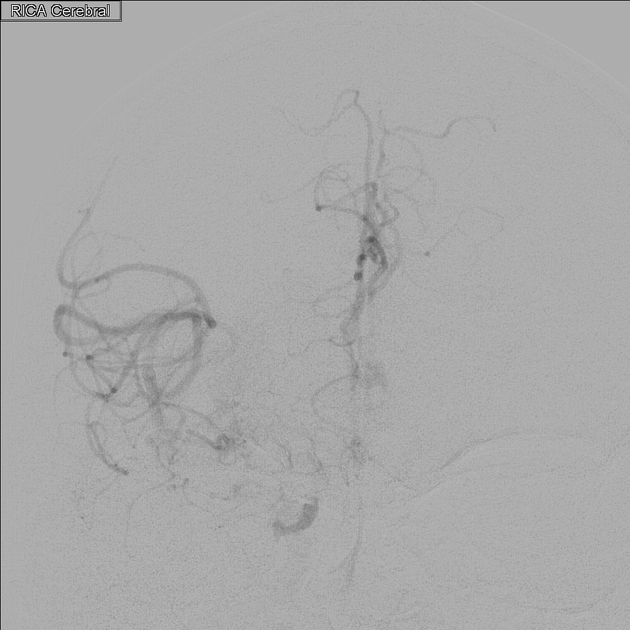
Supply from the right meningohypophyseal trunk to the right caroticocavernous fistula with retrograde opacification of the superior orbital vein.
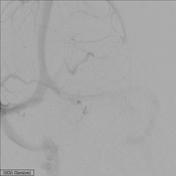
Normal right external carotid artery branches without supply to the caroticocavernous fistula.
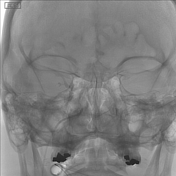
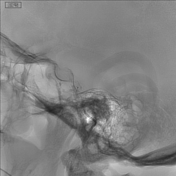
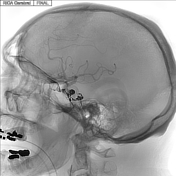
Opacification of right cavernous sinus noted, with likely previously partially thrombosed right inferior petrosal sinus and portions of the cavernous sinus. Venous microcatheter injections into the cavernous sinus confirm the caroticocavernous fistula anatomy visualized by right internal carotid artery injections, with eventual microcatheter position wedged into venous side of caroticocavernous fistula. Final images show Onyx cast in an appropriate position within cavernous sinus where the caroticocavernous fistula existed prior to embolization.
Right ICA angiogram after transvenous embolization with Onyx-18 demonstrates no opacification of the cavernous sinus.
CONCLUSION: Right caroticocavernous fistula supplied by the right meningohypophyseal trunk (Barrow type B); successfully embolized transvenously with Onyx-18.
Case Discussion
55-year-old male with rapidly progressive right eye proptosis, chemosis, visual loss and orbital compartment syndrome due to a spontaneous Barrow type B indirect caroticocavernous fistula (shunt between meningohypophyseal trunk, an intracavernous branch of the internal carotid artery, and cavernous sinus). The patient initially was treated with antibiotics and steroids with no response. CTA and MRI findings suggested a caroticocavernous fistula. The patient underwent emergent lateral canthotomy with cantholysis and subsequent transvenous embolization of the caroticocavernous fistula Onyx-18 with symptomatic relief and residual blepharoptosis 9 months after treatment. The patient is planned for 9 mm right internal levator advancement for the treatment of blepharoptosis in the future.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.