
Presentation
Atypical chest pain. History of smoking and hyperlipidemia.
Patient Data



Technique
patient premedication: beta blocker and nitrates
acquisition method: step and shoot (prospective acquisition - 100 KV)
contrast injection protocol: triphasic injection
image reconstruction: standard without edge correction
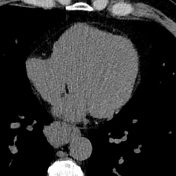
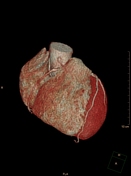
Findings
normal coronary origins
balanced coronary arterial dominance
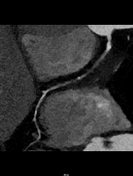
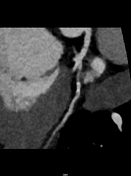
long occluded segment of the right coronary artery
Plaque burden:
calcium score (according to Agatson, not shown): 104
segment involvement score: 3-4
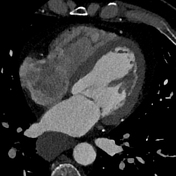
Right coronary artery (RCA): double distal segment
high-grade stenosis in the proximal segment with subsequent segmental occlusion of the distal proximal and middle segments
the doubled distal segment is being fed via collaterals
Left main: inconspicuous
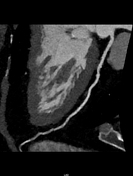
Left anterior descending artery (LAD): two diagonal branches
eccentric mixed plaque in the proximal segment without significant stenosis
thin, rudimentary first diagonal branch
strong second diagonal branch without stenosis
stair step artifact in the distal segment
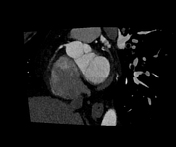
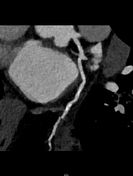
Circumflex artery (CX): two marginal branches (OM1 & OM2) and posterolateral branch
eccentric calcified plaque of the proximal segment
thin first marginal branch with at least moderate stenosis proximally (D: 50-69%)
no plaques or stenosis of the second marginal and posterolateral branches
stair step artifact in the distal segment
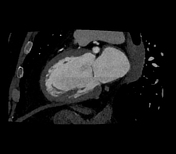
Impression
chronic occlusion of the right coronary with distal collateralisation
proximal moderate stenosis of a thin first marginal branch
moderate amount of coronary plaque
CAD-RADS 5/P2
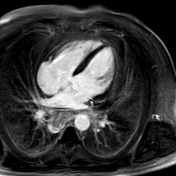
massive bilateral hilar and mediastinal lymphadenopathy
Exam courtesy: Silva Reinecke (medical imaging technologist)
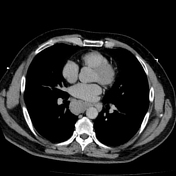



Massive bilateral hilar and mediastinal lymphadenopathy.
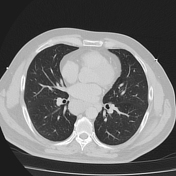
No lung mass was detected.
Mild emphysema.





Heart rate: ~70 bpm at rest -> 90 bpm during stress perfusion after Adenosin 140 µg/kg/min
Image quality: mild to moderate respiratory artifacts, otherwise no limitations
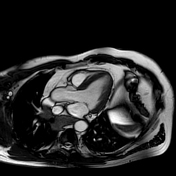
Morphology and functional analysis (endo-volume):
LV-EDVI: 75 mL/m²
LV-ESVI: 38 mL/m²
LV-SVI: 37 mL/m²
LV-EF: 49%
cardiac output: 5.8 L/min
cardiac index: 2.6 L/min/m²
LV-ED wall mas index (without papillary muscles): 67 g/cm
septum and inferior wall thickness: 9 and 8 mm
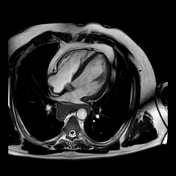
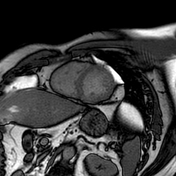
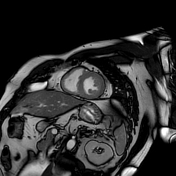
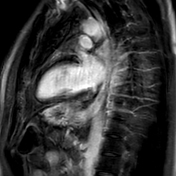
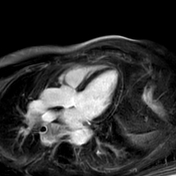
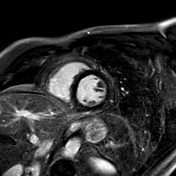
Findings:
Mild hypokinesia in basal inferoseptal and inferior segments.
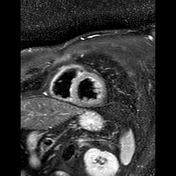
No evidence of focal myocardial edema on STIR.
Mildly elevated T1 mapping values in septal and inferior segments (z-score: 2-3).
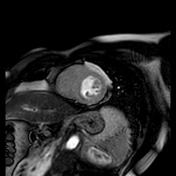
Small subendocardial perfusion defect under Adenosin stress in inferoseptal and inferior midventricular segments not visible during rest.
No intracavitary thrombi.
Impression:
Cardiac MRI findings are consistent with mild myocardial ischemia in midventricular inferioseptal and inferior segments.
Norma viability of the myocardium. No signs of infarction or myocardial scar tissue.
Mildly elevated T1 mapping values possibly mild myocardial edema.
Exam courtesy: Jeanette Moses & Tobias Jahn (medical imaging technologists)
Case Discussion
A case of a patient with chronic occlusion of the right coronary artery with mild myocardial ischemia and partial collateralisation via branches of the circumflex artery. Myocardial viability is preserved with no signs of myocardial infarction or myocardial scar tissue.
The RCA occlusion was confirmed by cardiac catheterization, which also showed the collateral pathway via branches from the circumflex artery. The stenosis of OM1 was not significant.
Based on these findings, the patient is very likely to benefit from revascularization 1 and was therefore transferred to a cardiac center.
The bilateral hilar and mediastinal lymphadenopathy is further investigated oncologically.
Courtesy: Dr Soeren Linsel (cardiologist)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.