
Presentation
The patient presented to the emergency department with severe abdominal pain and vomiting. On examination, the abdomen was rigid and tender with palpable mass at the right upper abdomen.
Patient Data
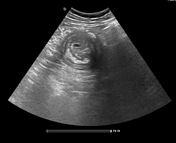

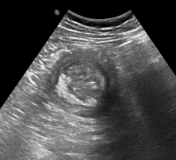

Thickened bowel loop with target (doughnut) sign and hyperechoic crescent-in-doughnut sign at the right upper abdomen.
Large nearly rounded intraluminal hyperechoic focal lesion with a little bit posterior shadowing.
Few echogenic foci at the peripheral aspect of the thickened bowel wall suggesting intramural air.
Gallbladder shows comet-tail artifact suggesting adenomyomatosis.
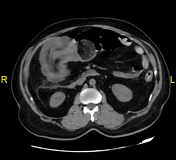
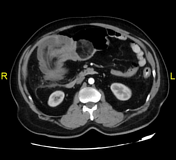
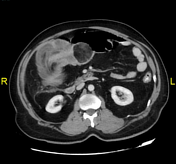
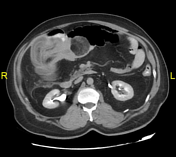
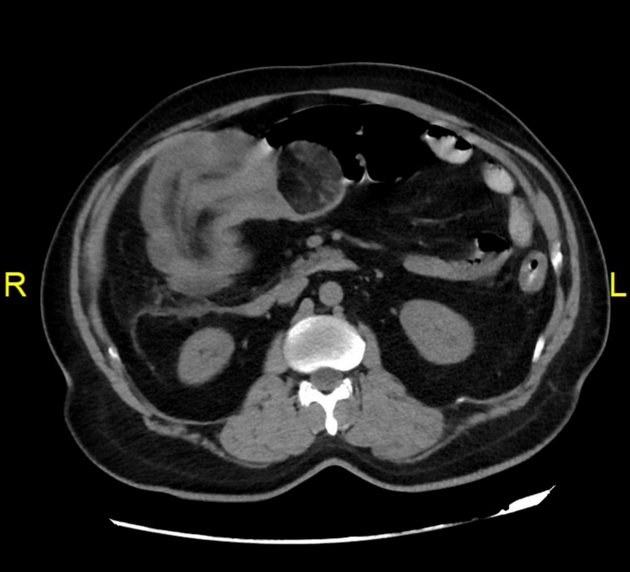
Severely thickened edematous hepatic flexure with intraluminal invaginated ascending colon giving telescope sign.
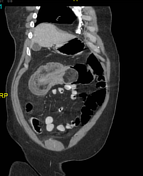
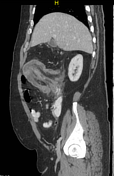
Well define intraluminal fatty lesion at the distal aspect of the lesion in the transverse colon suggesting colonic lipoma.
Few intramural gas locules (coronal, sagittal).
Few mildly enlarged mesenteric lymph nodes.
Case Discussion
Colocolic intussusception is a specific type of intussusception where a segment of the colon telescopes into an adjacent segment of the colon.
In adults, colocolic intussusception is often associated with a pathological lead point, such as a tumor (benign or malignant), polyp, or diverticulum.
The complications of intussusception are bowel obstruction, ischemia and necrosis of the affected bowel, and perforation and peritonitis if untreated.
Our case is a typical case of colocolic intussusception secondary to colonic lipoma with characteristic target (doughnut) sign, crescent-in-doughnut sign, and telescope sign.
The patient underwent emergency surgery that confirmed colocolic intussusception, with the presence of a mass as a leading point which was confirmed to be a lipoma after that by pathological examination.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.