
Presentation
Fever and odynophagia. Trip to Italy 7 days ago. Low oxygen saturation (SpO2 89%) and lymphopenia were observed. The patient presented clinical worsening during his stay in the emergency department, and radiological control was performed at 12 hours. SARS-CoV-2 RNA was detected.
Patient Data
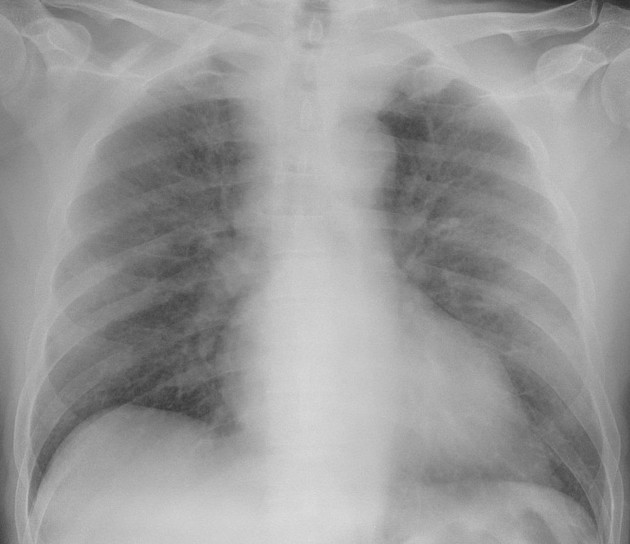
Faint, ill-defined alveolar consolidations in both upper lobes.

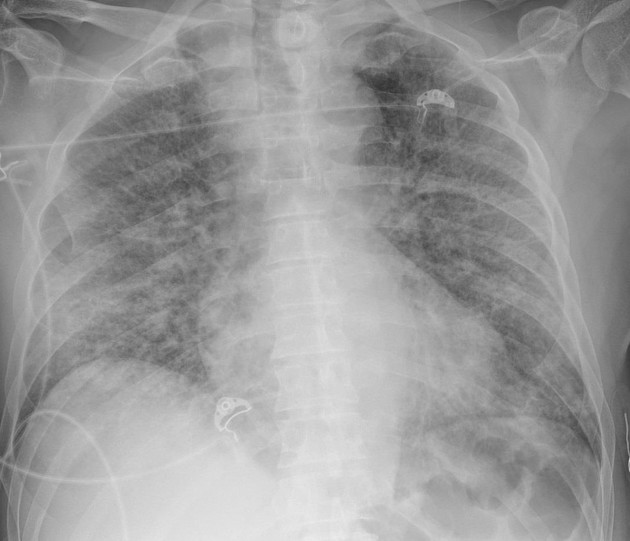
Radiological worsening with patchy, bilateral alveolar consolidations with panlobar opacities, suggesting ARDS secondary to COVID19.
Radiological stability, with slight improvement of the alveolar consolidation in right lower lobe. The patient still needs supportive care measures.
Case Discussion
SARS-CoV-2 infection (COVID-19) can lead to rapidly progressive ARDS as shown in this case. The prognosis is poor and radiologic findings can go from ill-defined alveolar consolidations to bilateral consolidations with panlobar changes as seen in ARDS.
Radiographic and computed tomography (CT) imaging early in the disease course may be normal; chest CT has been described as more sensitive than chest x-ray for the detection of characteristic bilateral, peripherally-predominant ground-glass opacities. However, the patient's clinical situation often does not allow a CT scan.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.