
Presentation
Headache, right-sided weakness, and decreased level of consciousness for two weeks and nausea for two days. No vomiting, seizures, or fever.
Patient Data



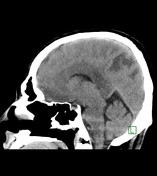
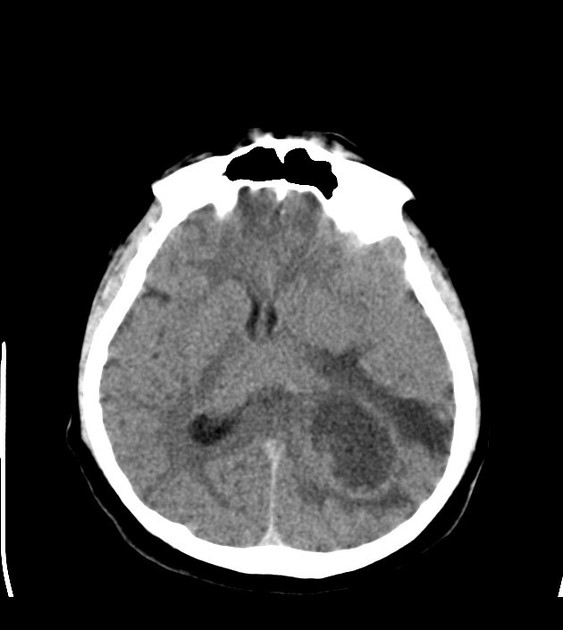
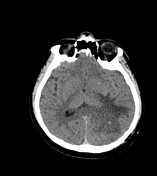
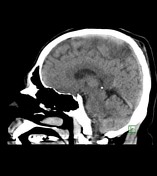
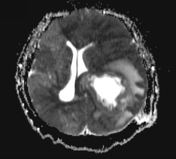
A rounded ring-like structure (with peripheral hyperdense rim and hypodense center) measuring 4.8 x 5.3 cm (axial image), surrounded by prominent vasogenic edema and significant mass effect on the surroundings (effacement of the adjacent cortical sulci, obliteration of the atrium & occipital horn of the left lateral ventricle, obliteration of the quadrigeminal cistern, and 8 mm midline shift to the right side) is seen in the left parietal region. The lesion shows questionable extension along the splenium of the corpus callosum. These findings are highly suggestive of an aggressive neoplastic lesion (high-grade glioma). Another possible differential is brain abscess which is, however, less likely. For further evaluation with MRI brain.
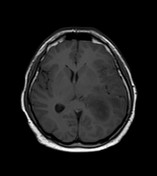
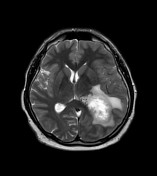

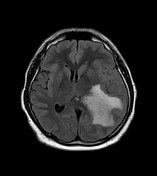
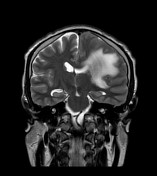
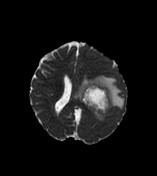
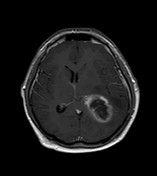
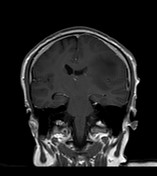
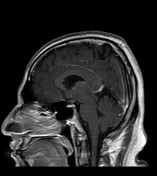
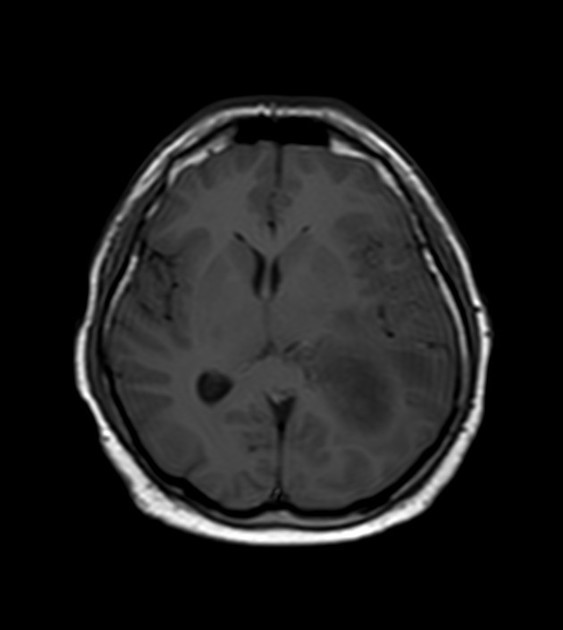
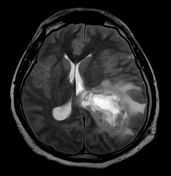
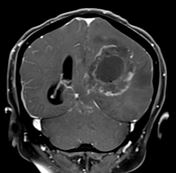
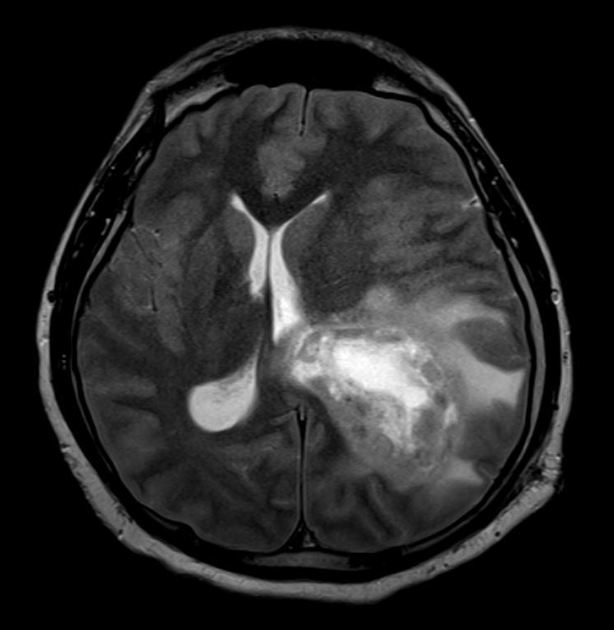
An intra-axial cystic lesion measuring approximately 5 cm is seen in the left posterior parietal lobe. It has thick peripheral walls/capsule which enhances significantly on post-contrast images. Perilesion vasogenic edema, the mass effect over the left lateral ventricle, and mild uncal & subfalcine herniations. Diffusion-weighted images show mild restriction in the wall of the lesion; however, no restriction is seen in the center of the lesion. MR spectroscopy revealed elevated choline, elevated choline creatine ratio, and markedly depressed NAA peaks. The overall picture is suggestive of a high-grade tumor, like glioblastoma multiforme (GBM). Another possible differential is the cystic brain metastasis, which is, however, less likely. For pathological correlation.
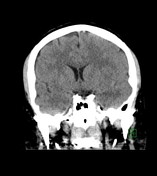

Status post left parietal craniotomy. A heterogeneous cystic space-occupying lesion is seen in the left parietal lobe which has been partially aspirated; it now measures 3.8 x 4.5 cm as compared to the previous measurement of 4.8 x 5.3 cm (axial image). Its hyperdense peripheral walls which were relatively smooth in outline (on the previous scan) now have become irregular which is likely related to the partial aspiration and biopsy. No gross interval change is appreciable in the perilesional vasogenic edema and mass effect in the adjacent brain parenchyma. Interval improvement is seen in the right-sided midline shift which now measures 5 mm (as compared to the previous measurement of 8 mm).
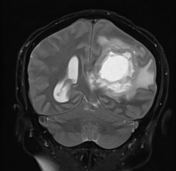
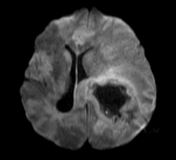
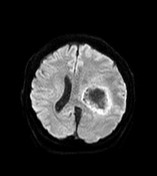
A large cavitating tumor with a thick wall measuring about 6.1 x 5.3 cm, associated with surrounding vasogenic edema, significant mass effect, extension into the left lateral ventricle, and uncal & subfalcine herniations, is seen in the left parietal lobe. Multiple foci of hemorrhagic components and new vasculature related to the underlying high-grade tumor, are seen in the wall of the lesion in the gradient-echo images. Abnormal nodular enhancement is seen in the tumor wall on post-contrast images. Restricted diffusion (ischemic stroke) is seen in the whole left cerebral hemisphere as well as in the right ACA & MCA territories, which is most likely related to the mass effect on the vasculature, caused by the uncal and subfalcine herniations. MR spectroscopy shows a high choline-creatine ratio.


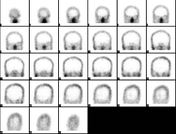
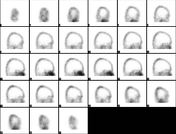






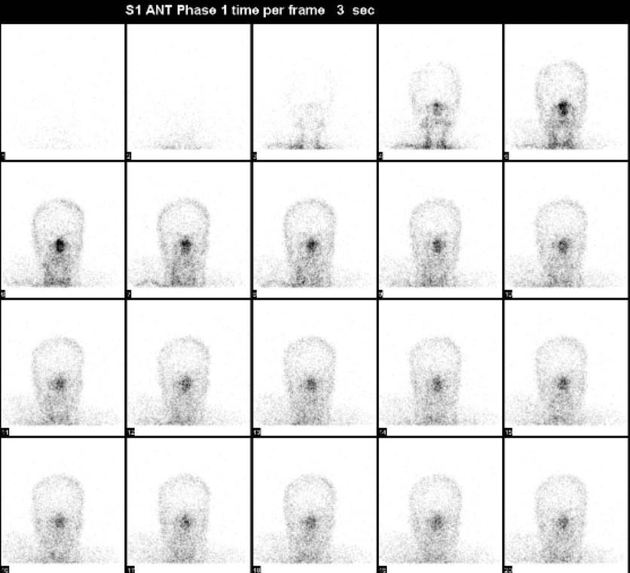
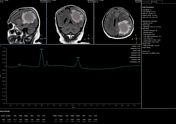
Tc-99m Ceretec Tc-99m HMPAO Hexamethylpropylene cerebral perfusion scan
No intracranial uptake/cerebral perfusion (empty light bulb sign) is seen, which is consistent with brain death. Relatively increased perfusion is seen in the nasal region due to the preserved external carotid artery flow (hot nose sign).
Case Discussion
-
The patient underwent left parietal craniotomy with incisional biopsy and aspiration of fluid contents of the left parieto-occipital cystic brain mass.
- Analysis of aspirated fluid contents from the cerebral lesion: Atypical and necrotic cells.
Histopathology of incisional biopsy: High-grade glioma (grade III according to the WHO classification). However, the histological features of high-grade glioma, in combination with necrosis found in the aspirated fluid contents, are in favor of glioblastoma (grade IV according to the WHO classification).
The immunostain with the antibody anti-GFAP is positive in the atypical cells. Immunostain with the antibody anti-p53 shows strong nuclear positivity in the infiltrative and scattered tumor cells. The immunostain with the antibody anti-Ki67 is positive in about 20% of tumor cells. The antibody anti-pan cytokeratin (AE1/AE3) is negative. IDH1/2 mutation analysis (RT-qPCR) shows no mutation.
Final diagnosis: Glioblastoma, IDH-wild type, WHO grade IV.
The patient’s general clinical condition deteriorated very rapidly after biopsy (development of seizures and dropping GCS level). Last imaging (MRI brain) showed progressive disease with extensive ischemic changes in bilateral cerebral hemispheres (L>R) and brain death on cerebral perfusion scan. The patient expired within 6 weeks of his initial presentation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.