
Presentation
Vague intermittent lower abdominal pain. Referred by gynecology for MRI following sonographic detection of a large adnexal mass. Normal labs.
Patient Data

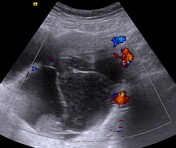
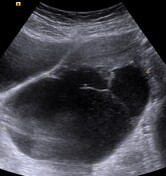

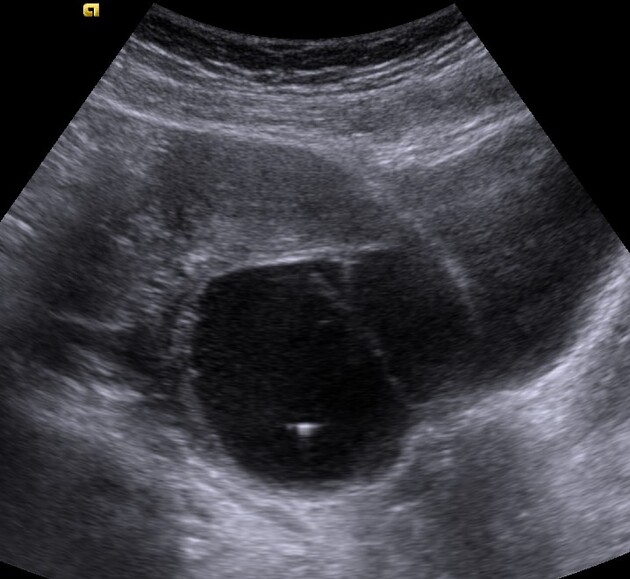
Large lobulated multilocular left adnexal cystic lesion with posterior acoustic enhancement occupying the posterior cul-de-sac, Likely arising from the left ovary, containing a small avascular intralesional papillary projection and echogenic internal debris, a few of which exhibit comet tail artifacts. The right ovary was separately identified (not shown).



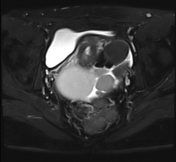
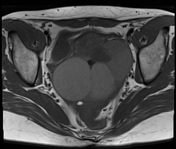
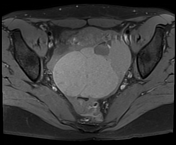

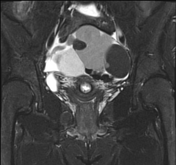

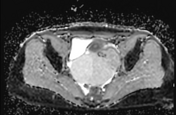
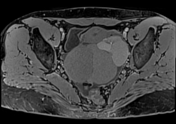
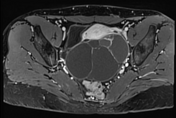
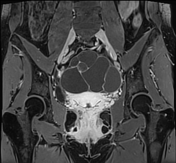
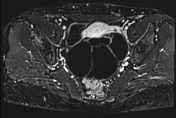

Large predominantly cystic left adnexal mass occupying the rectouterine space, compressing and anteriorly displacing the uterus and right adnexa. It contains multiple cystic locules of variable sizes and varying (high and low) signal intensity on all sequences. No intralesional fat or enhancing solid components. A thick enhancing wall is demonstrated following contrast administration, with a smooth weblike (lacy) pattern of enhancement corresponding to internal septations, which exhibit restricted diffusion on DWI.
It appears to be drained by the left ovarian vein. The stroma of the left ovary is not visualized (phantom organ sign). These findings indicate a left ovarian origin.
Moderate amount of pelvic free fluid. No suspicious pelvic lymphadenopathy. No localized collections.

A complimentary unenhanced CT scan of the pelvis -obtained following MRI- revealed a complex pelvic mass occupying the rectouterine pouch, composed of multiple high-density cystic locules of variable sizes, with no intralesional fat or calcification.
Minimal excreted gadolinium in both distal ureters.
A left ovarian cystectomy was performed. Histopathological assessment revealed thyroid tissue lining with focal hyperplasia and multiple colloid follicles of variable sizes.
Case Discussion
Struma ovarii should be suspected whenever encountering a complex multiloculated lobulated cystic ovarian mass with multiple cysts of varying signal intensity, sizes and a lacelike pattern of enhancement 1-4.
The comet tail artifact seen on ultrasound, as well as the variable signal intensity on MRI, were consistent with gelatinous intralesional colloid.
Struma ovarii is a rare, usually benign ovarian monodermal teratoma predominantly consisting of thyroid follicular tissue and colloid contents. 5-10% of struma ovarii tumors are reported to be malignant, histopathologically revealing papillary thyroid carcinoma 1.
Most are discovered incidentally as the majority of lesions are asymptomatic, unless the tumor is very large, resulting in ovarian torsion. Around 5% of struma ovarii patients may present with signs of thyrotoxicosis. Ascites and elevated CA 125 may also be encountered 1.
Our patient's thyroid function test and tumor markers were normal.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.