
Presentation
The patient presented with ankle pain and swelling.
Patient Data
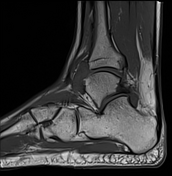

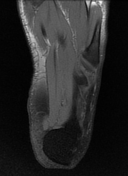
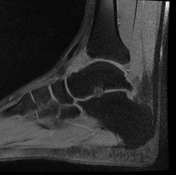
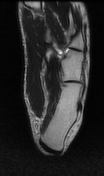
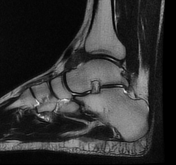
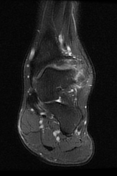
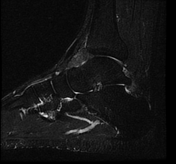

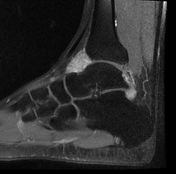
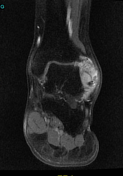

Globular mass-like synovial thickening extending to the anterior and posterior ankle joint recesses and encasing the anterior talofibular ligament. It elicits isointense signal to muscles on T1 with internal hypointense foci and hypointense capsule, low signal on T2, intermediate signal on PDFS/STIR, and shows intense enhancement after intravenous contrast (axial, sagittal. coronal).
Peroneus quartus muscle (an accessory peroneus muscle) (axial, sagittal, coronal).
Small accessory soleus muscle (axial, sagittal, coronal).
Case Discussion
A diffuse tenosynovial giant cell tumor (D-TSGCT), formerly known as pigmented villonodular synovitis (PVNS), is a rare, benign but locally aggressive tumor that affects the synovial lining of joints, bursae, or tendon sheaths. It is often leading to joint damage and functional impairment if left untreated.
T2 hypointense lesions on MRI with “blooming” from hemosiderin deposition on SWI/GRE images are virtually pathognomonic of this disease.
Unfortunately SWI/GRE wasn't done in our case, but the hypointense T2 signal highly suggest diffuse tenosynovial giant cell tumor (D-TSGCT).
The peroneus quartus is an accessory peroneus muscle. It typically descends medial and posterior to the peroneal tendons. The muscle is name the fourth peroneal because the name peroneus (fibularis) tertius which is not a lateral (peroneal) compartment muscle, as it runs with the extensor digitorum longus in the anterior compartment of the leg to insert on the dorsal surface of the base of the fifth metatarsal.
Also, our case shows small accessory soleus muscle which is a rare congenital supernumerary anatomical variation of the lower leg.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.