
Dysphagia lusoria from aberrant left subclavian artery with Kommerell diverticulum
Presentation
Long-standing dysphagia and reflux. No other past history.
Patient Data
Barium swallow



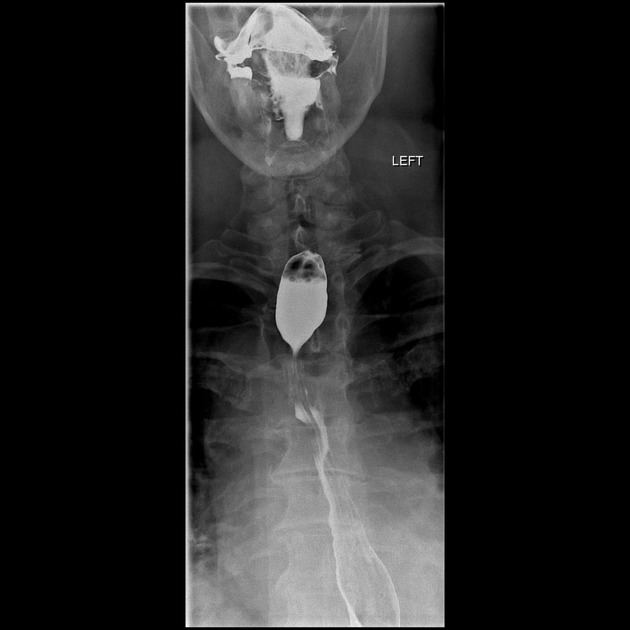
Smooth posterolateral indentation of the proximal thoracic esophagus suggesting extrinsic compression.
Courtesy of Dr Calvin Gan.
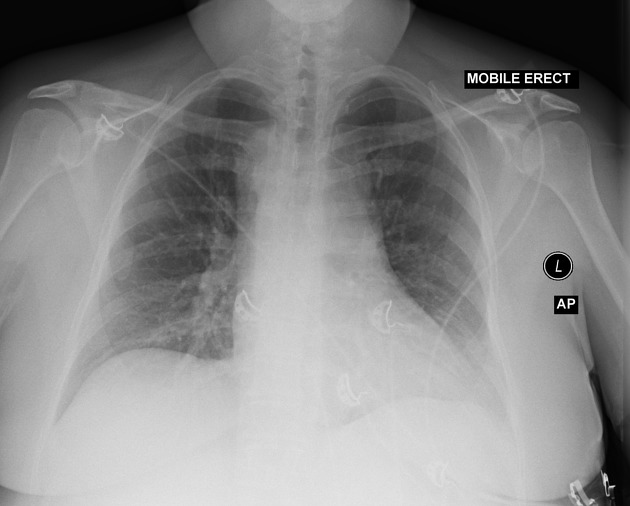
Right aortic arch, otherwise cardiomediastinal contour is normal. Lungs and pleural spaces are clear.


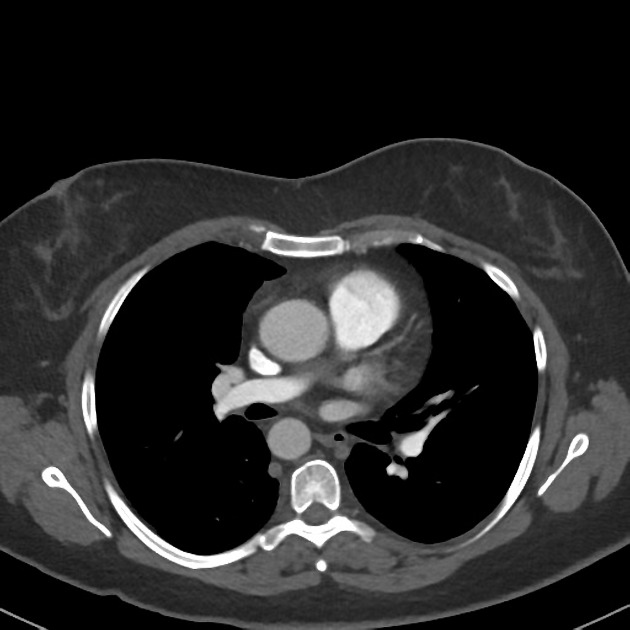
Right aortic arch with retro-esophageal aberrant left subclavian artery. Dilatation of its origin, consistent with a Kommerell diverticulum.




Right aortic arch with Kommerell diverticulum. TEVAR from proximal aortic arch to mid descending thoracic aorta. Previous ligation of the first part of an aberrant left subclavian artery with left common carotid to left subclavian bypass. Peripheral filling of the Kommerell diverticulum is noted with a central filling defect.
Left upper lobe airspace opacity.
Case Discussion
This is a symptomatic aberrant left subclavian artery with Kommerrell diverticulum has been treated in a two-stage hybrid approach. Initially the a carotid-subclavian bypass was performed, and this was followed by exclusion of the Kommerell diverticulum with a TEVAR.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.