
Presentation
Patient fell and sustained a pertrochanteric fracture, treated with an intramedullary nail. Post op x-rays of femur were obtained to assess position.
Patient Data



The pertrochanteric left femoral fracture has been fixed with a long intramedullary nail and no periprosthetic complication noted (not shown). There is a single distal cross bolt in good position. Again noted is made of the 18 mm coarse clump of calcification, seen on the lateral radiograph and thought to be within the lateral femoral condyle.


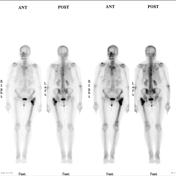
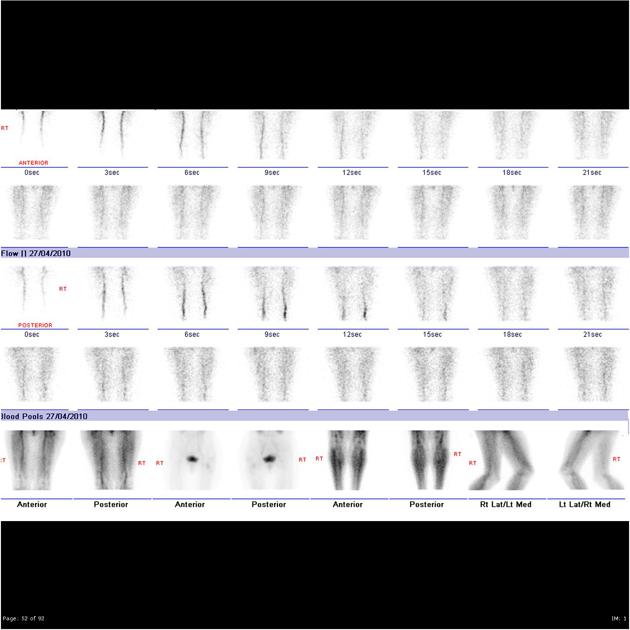
Initial blood flow studies of the knees and thighs show slightly increased vascularity at the left upper femur. Delayed whole body study and multiple views of the femur show an intense increase in tracer uptake at the upper end of the left femoral shaft particularly at the lesser trochanter. This is consistent with the recent fracture though the intensity at the lesser trochanter appears excessive (? delayed union).
In the lower femoral shaft the supracondylar region (distinct from the screw induced cortical lesions) only a minor increase in tracer uptake is noted consistent with a metabolically inactive lesion.
Elsewhere there is evidence of mild spondylosis at the right side of the lower lumbar spine and the right T7 and T8 consistent with spondylosis. The left renal upper half cortical filling defect is noted presumably a cyst but other lesions cannot be excluded. Minor increases in tracer uptake are noted at the acromioclavicular joints consistent with osteoarthritis there or underlying supraspinatus tendinitis.




There is an irregular sclerotic lesion in the lateral metaphyseal region of the left distal femur measuring 11 x 14 x 11mm. No cortical breakthrough, endosteal scalloping or periosteal reaction. No soft tissue mass.

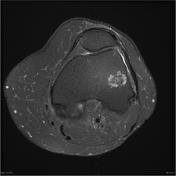
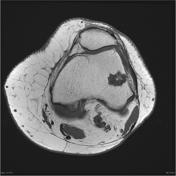
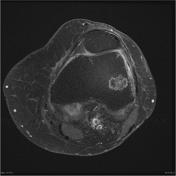
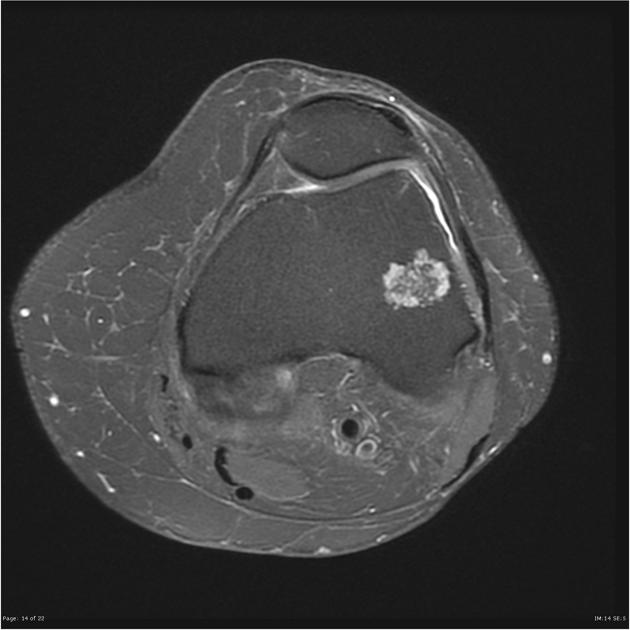
The lesion in the lateral femoral condyle shows no marrow reaction, has a multilocular appearance and shows typical rim enhancement, with central low signal on all sequences (due to calcification) admixed with high T2 low T1 signal material.
Distal end of femoral intramedullary rod noted.

Distribution of enchondromas. Layout and distribution: Frank Gaillard 2012, Line drawing of skeleton: Patrick Lynch 2006, Creative Common NC-SA-BY
Case Discussion
Features are typical of a low grade chondral lesion, almost certainly an enchondroma. The patient has been followed up for 18 months and this lesion has remained stable.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.