
Enchondromas, also known as chondromas 7, are relatively common intramedullary hyaline cartilage neoplasms with benign imaging features. They share histologic features with low-grade chondrosarcoma and are sometimes classified under the umbrella term low-grade chondral series tumors.
Enchondromas account for the 'E' in the popular mnemonic for lytic bone lesions FEGNOMASHIC.
On this page:
Epidemiology
most frequently diagnosed in childhood to early adulthood with a peak incidence of 10-30 years
account for ~5% (range 3-10%) of all bone tumors and ~17.5% (range 12-24%) of benign bone tumors 1
Associations
Two syndromes are associated with multiple enchondromas:
Diagnosis
Diagnosis of enchondroma is typically based on radiological features alone.
Diagnostic criteria
Diagnostic criteria according to the WHO classification of soft tissue and bone tumors (5th edition) 12 are:
abundant cartilaginous matrix
-
absence of:
cellular atypia/mitoses
soft tissue extension
cortical invasion
Clinical presentation
Enchondromas are most commonly an incidental finding, most significant in that they should not be confused with more aggressive lesions.
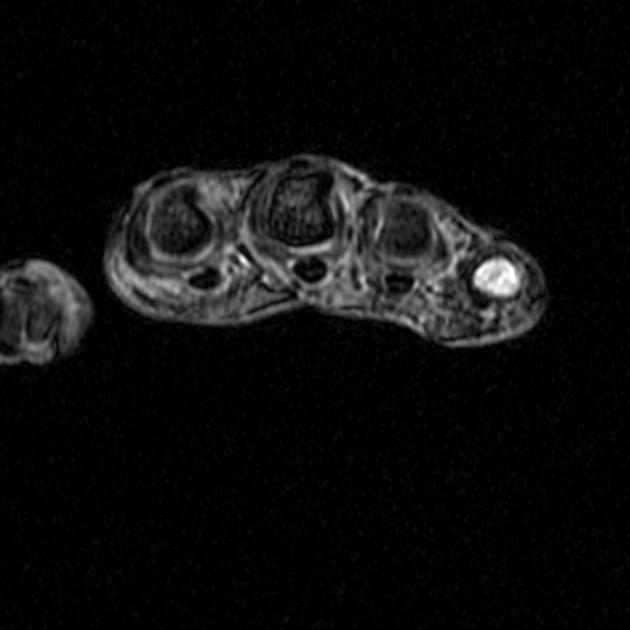
As a rule, enchondromas should be asymptomatic; however, lesions of the hands/feet may present with pain from pathological fracture or impending fracture 8.
Malignant transformation into low-grade chondrosarcoma is rare and may present with pain.
Pathology
Enchondromas comprise lobules of mature hyaline cartilage which are partially or completely encased by surrounding normal bone 9. The cartilaginous lobules may undergo endochondral ossification, often resulting in the characteristic 'rings and arcs' pattern of mineralization.
They arise from the rests of the growth plate cartilage/chondrocytes which become isolated within the mature bone. Hence, they may be seen in any bone formed from cartilage.
By definition, they show no histologic evidence of local invasion (which would suggest low-grade chondrosarcoma). However, it is important to be aware that enchondroma cannot be reliably distinguished from chondrosarcoma 13 by histology, and diagnosis depends on the correlation of clinical, imaging, and pathology findings 9.
Grossly, lesions are usually <3 cm, translucent, nodular, and grossly grayish-blue.
Location
Enchondromas are typically located in a central or eccentric position within the medullary cavity of tubular bones:
-
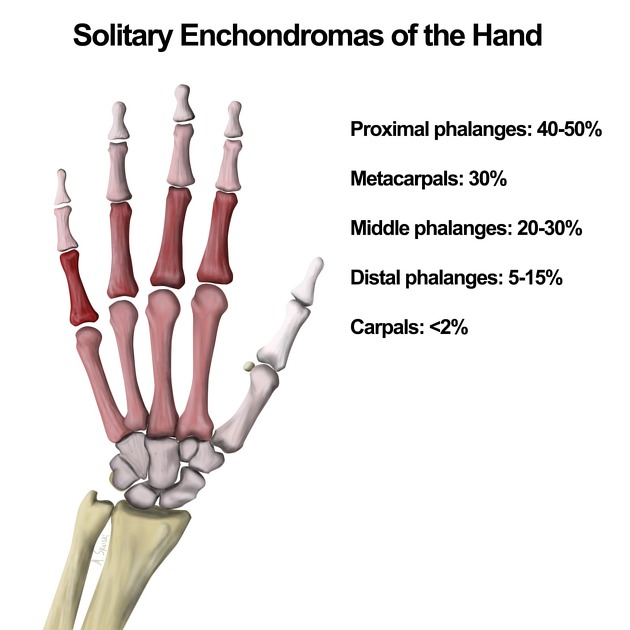
small tubular bones of the hands and feet (~50%) 4
proximal phalanx most common 8
-
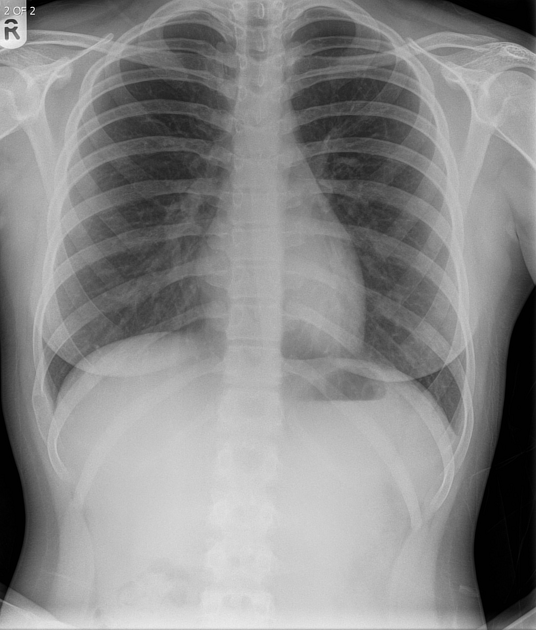
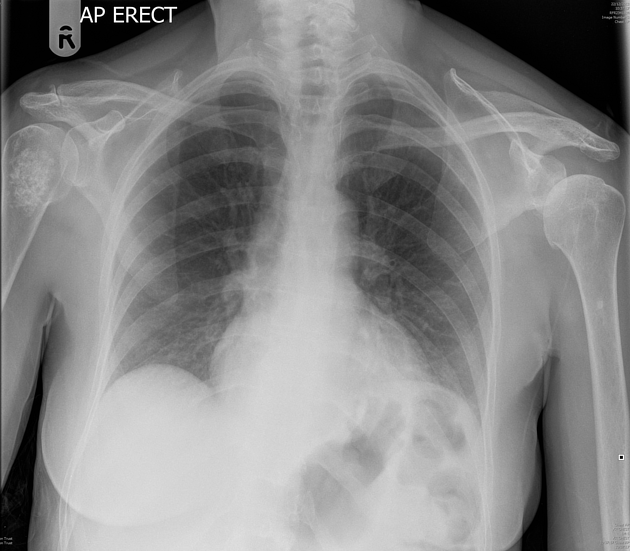
large tubular bones
e.g. femur, tibia, humerus
-
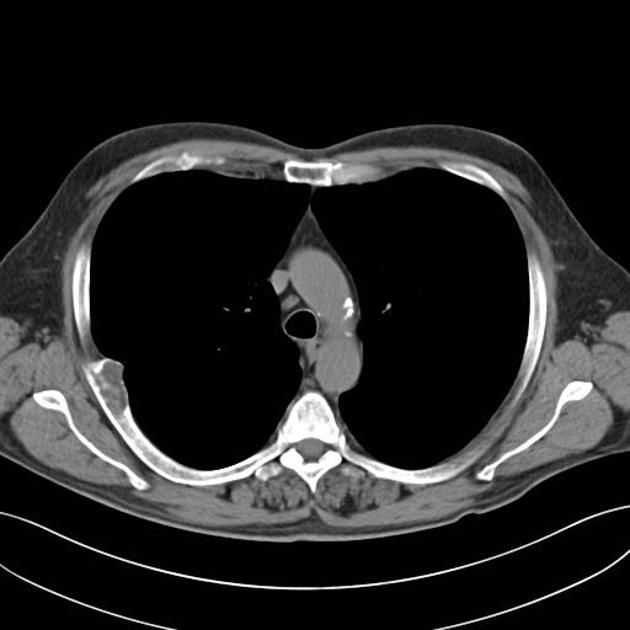
rare: (consider chondrosarcoma)
pelvis
ribs
sternum
Rarely an enchondroma may extend through the cortex and demonstrate an exophytic growth pattern. This is known as an enchondroma protuberans and may either be seen sporadically or as part of Ollier disease 2.
Radiographic features
Enchondromas have a somewhat variable appearance by imaging, although characterization by excluding suspicious features is critical. Since most are asymptomatic incidental findings, lesions in a characteristic location and appearance are not usually further investigated.
Imaging is generally less helpful in corroborating the benignity of lesions in the hands/feet, as well as in enchondromatosis or skeletally immature patients 9.
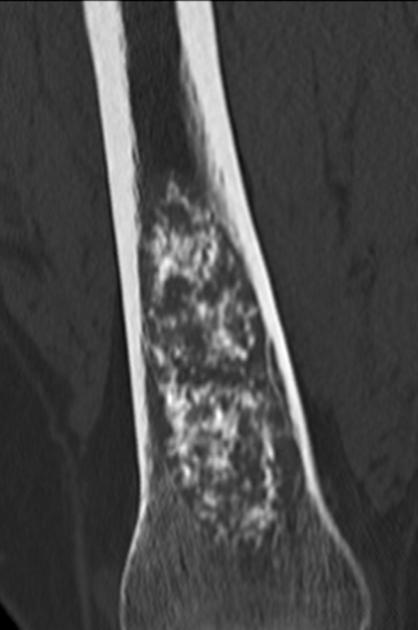
Plain radiograph and CT
Enchondromas have a variable appearance, although typically they are small <5 cm intramedullary lytic lesions with non-aggressive features:
a narrow zone of transition
sharply defined margins
-
+/- chondroid calcification (rings and arcs calcification)
often no matrix mineralization (purely lytic) in the hands/feet
-
+/- expansile
more commonly in hands/feet, less common in long bones (tibia, femur)
may have mild endosteal scalloping
should not "grow" through the cortex (unless a pathological fracture)
-
pertinent negatives 9
no gross bone destruction
no periosteal reaction
no soft tissue mass
Most enchondromas more frequently arise in the metaphyseal region, presumably due to their origin from the growth plate 1, although they are frequently seen in the diaphysis. They only rarely are seen in the epiphysis, and a cartilaginous lesion in an epiphysis is more likely to be a chondrosarcoma 3.
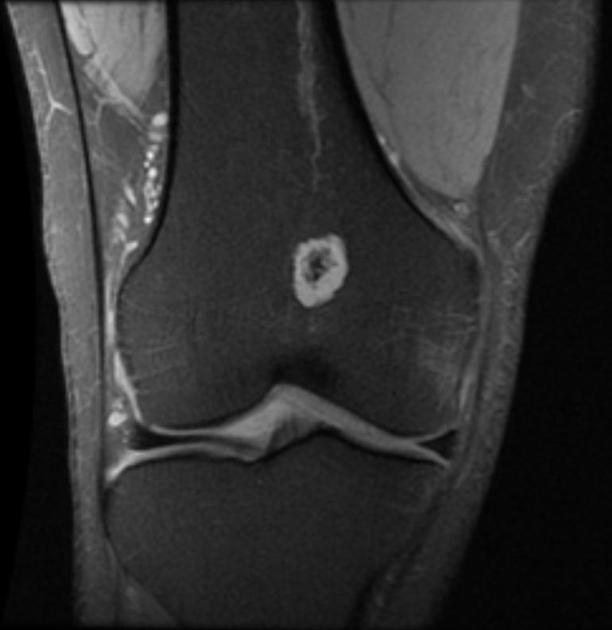
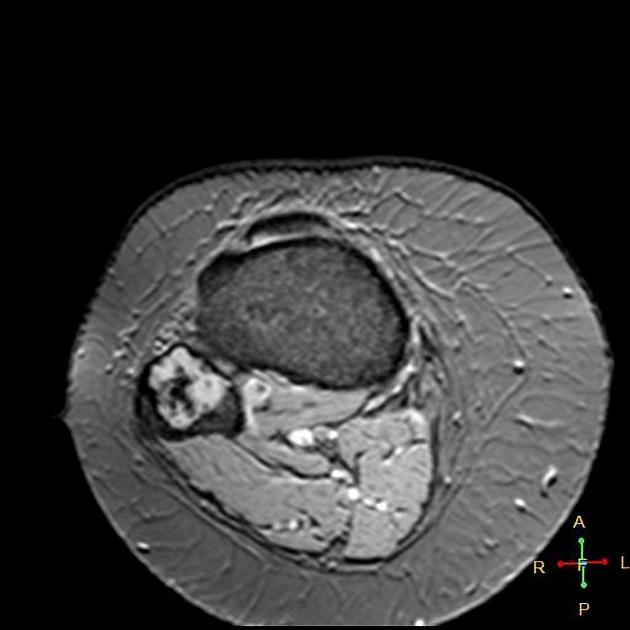
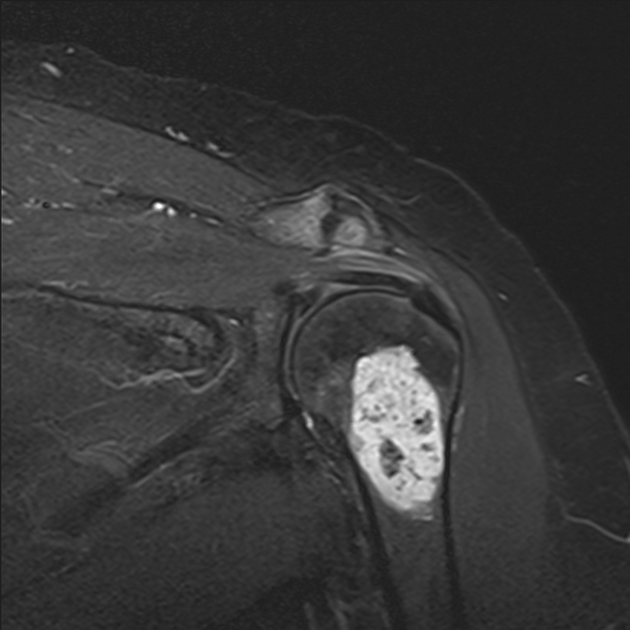
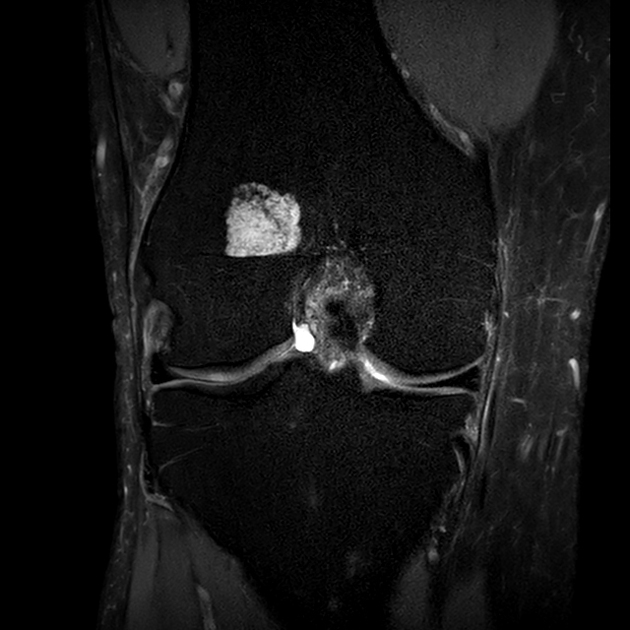
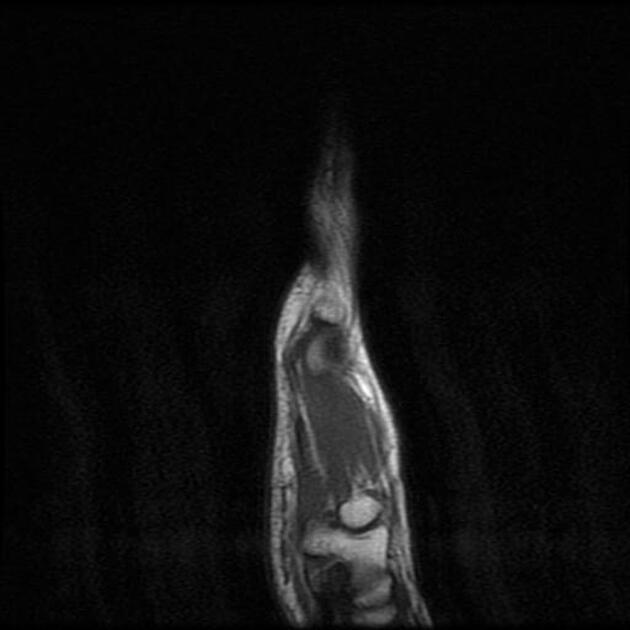
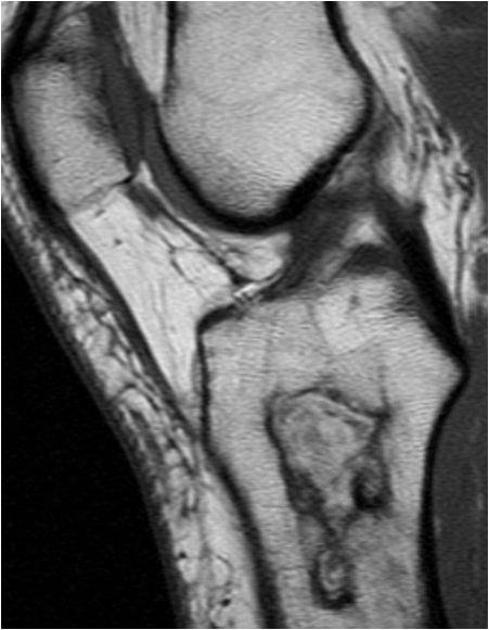
MRI
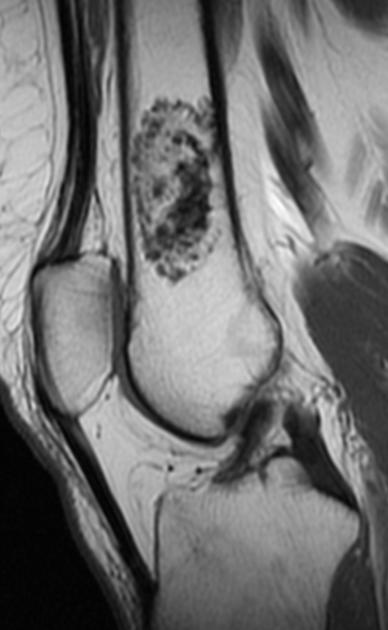
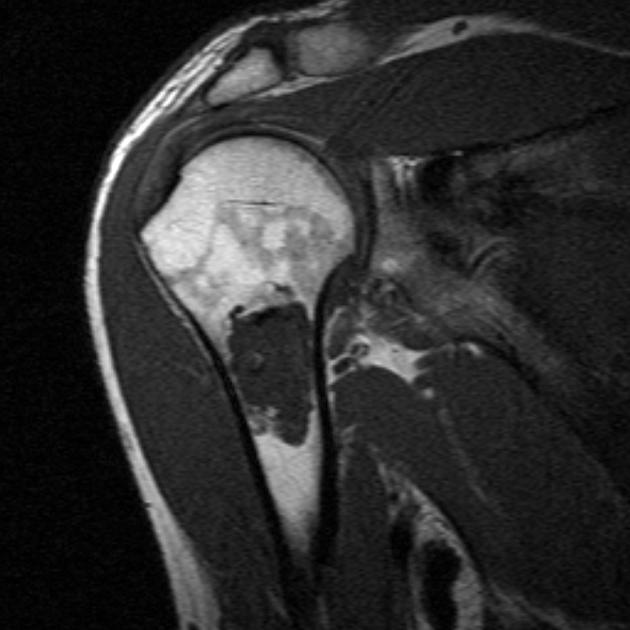
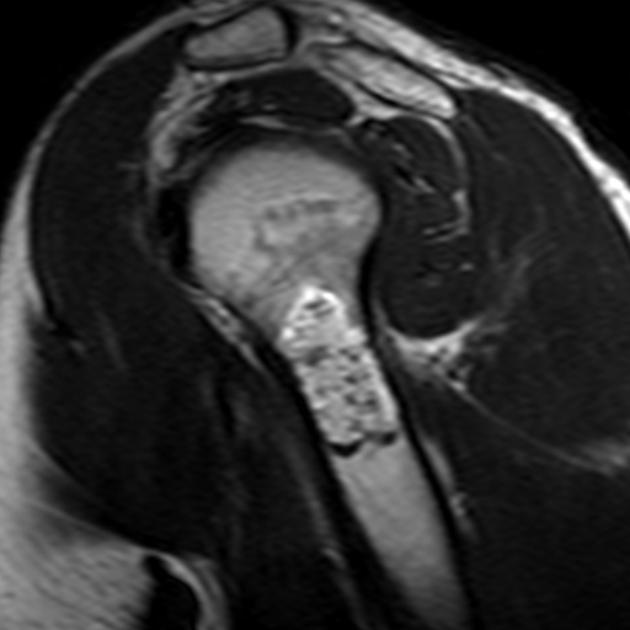
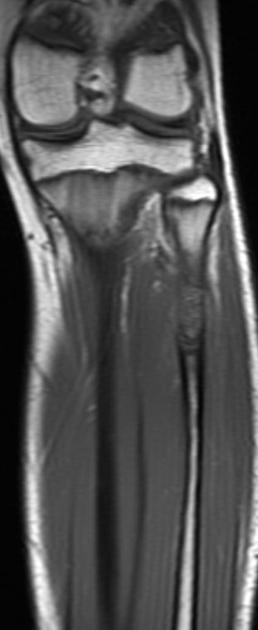
MRI is useful in evaluating soft tissue extension and confirming the diagnosis. Enchondromas appear as well-circumscribed, somewhat lobulated masses replacing marrow 1.
-
T1
intermediate to low-signal
internal foci of low signal of 'rings and arcs' characteristic of a chondroid matrix
-
T2
predominantly hyperintense and sharply defined - the cartilage is a hydrophilic tissue with high water content14
internal foci of low signal of 'rings and arcs' characteristic of a chondroid matrix
no bone marrow or soft tissue edema
-
T1 C+ (Gd)
enhancement of the scalloped margins with curvilinear translesional septa - rings and arcs enhancement6
a similar pattern of enhancement may be seen in chondrosarcomas 3,6
Differentiation of an enchondroma from low-grade chondrosarcoma is problematic, as they can have similar appearances. See enchondroma vs low-grade chondrosarcoma.
Nuclear medicine
Increased uptake on the bone scan can be seen with enchondromas. Intense uptake occurs with an underlying pathological fracture or cortical expansion in small bones 5.
Radiology report
The radiology report should include a description of the following:
location and size
tumor margins and transition zone
relation to the growth plate
presence of chondroid matrix
-
additional features:
cortical involvement, including endosteal scalloping
soft tissue extension
If the lesion is entirely consistent with an enchondroma with no concerning features, then it can be classified as Bone-RADS 1 11.
Treatment and prognosis
As enchondromas are classified as Bone-RADS 1 lesions, they are deemed to typically be benign and should be left alone if asymptomatic. The majority of enchondromas remain asymptomatic and require no treatment.
Pathologic fractures are commonly treated by curettage and bone grafting, with follow-up x-rays to monitor for healing and recurrence. An incisional biopsy is obtained intraoperatively. Recurrence is reported in 2-15% and suggests malignancy 8.
If malignant transformation is suspected, which occurs in less than 5% of cases, then treatment is more aggressive 4.
Complications
pathological fracture
malignant transformation into chondrosarcoma
Differential diagnosis
The differential is significantly affected by the modality in question, and most entities below can be excluded with MRI. The exception is chondrosarcoma.





















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.