
Presentation
Worsening dyspnea several months after rib fractures.
Patient Data





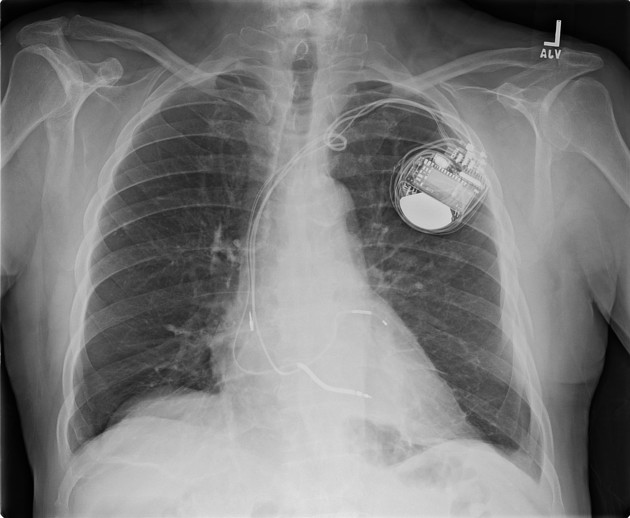
Displaced fractures of the lateral left 6-8th ribs. No effusion. No pneumothorax.
Subacute left rib fractures.
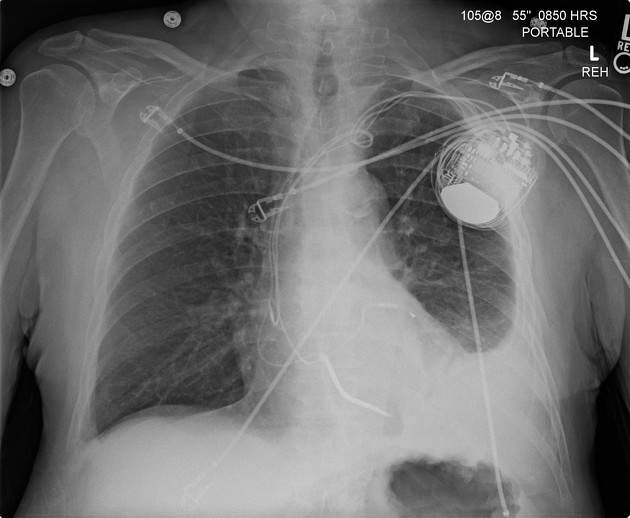
New left effusion with strandy retrocardiac and basilar opacity.





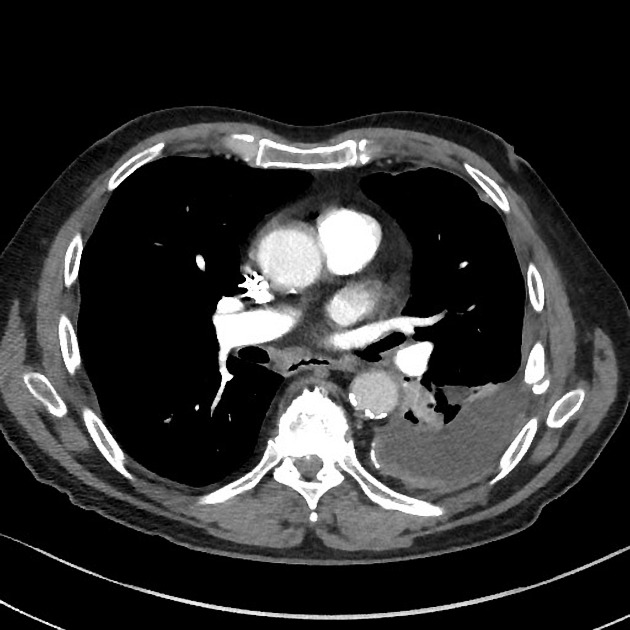
Medium sized left pleural effusion. Left pleural thickening with calcifications posteromedially. No right pleural calcifications (making asbestos an unlikely cause for the findings on the left). Collapse of the majority of the left lower lobe, with swirling/rounded appearance which can best be appreciated on the sagittal reformatted images. Moderate atelectasis of the lingula.
Incomplete healing of left 6-8th rib fractures.
Case Discussion
This is a very cohesive case which originally was unclear prior to the realization that this patient had recent rib fractures.
At the time of diagnosis of the rib fractures, no effusion was present. However, it is likely that the patient developed hemothorax which went untreated, particularly given the degree of displacement of the rib fractures. This is the most likely cause of the pleural thickening and calcification, which is only present in the left lung. There is medium-sized left effusion with significant collapse in the left lower lobe and lingula. The swirled appearance on the sagittal reformatted images is characteristic of rounded atelectasis, which is likely due to fibrosis of the visceral pleura.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.