
Presentation
Presented with abdominal pain, abdominal distension and no passing flatus for two days.
Patient Data



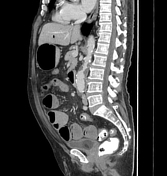
A large stone (14 x 22mm) is located at the distal ileum around 80mm from the ileocecal valve, causing proximal small bowel dilatation.
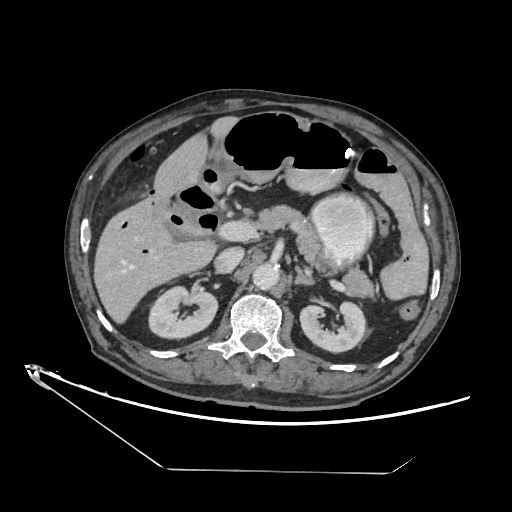
Numerous diverticula are seen at the sigmoid colon, descending colon, transverse colon and hepatic flexure. A calcified lesion is evident at the right paracolic gutter.
Diffuse pneumobilia of the dilated intrahepatic and extrahepatic ducts. The gallbladder is collapsed and thickened with intraluminal air locules and cholecystoduodenal fistula. Surrounding fat streakiness is noted.
A focus of calcification is seen in the pancreatic body. A renal cyst with no complex features is observed at the left upper pole.
There is encapsulated mesenteric fat streakiness with subcentimeter mesenteric lymph nodes seen at left sided abdomen.

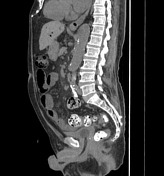


This current study no longer visualizes the large stone at the distal ileum. Small bowel dilatation has resolved. The rest of the findings are similar to those in the previous study.
Case Discussion
CECT abdomen findings are consistent with gallstone ileus and mesenteric panniculitis.
During the admission, the patient was kept NBM, and a nasogastric tube was inserted into the stomach. He was started on an IV drip and awaiting surgery if his condition did not improve clinically. After 3 days, he was able to pass flatus, and his abdomen became less distended. Repeated non-contrasted CT abdomen showed no stone or abnormal dilatation in the bowel loops.
The primary team assumed that the stone had been passed out spontaneously. His condition improved afterwards, and he was discharged well. The primary team will later arrange for elective surgery to repair the cholecystoduodenal fistula.
The stone impacted in the distal ileum was quite big! It is interesting because the stone passed itself without any medication or surgery.
Rigler triad of gallstone ileus includes 1,2:
ectopic gallstone in the small bowel loops, predominantly at the distal ileum
small intestinal obstruction


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.