
Presentation
Abdominal pain and dyspepsia.
Patient Data






A few small nodules, less than 4mm are scattered at both lungs which seems to be fibrotic nodules. There are also several atelectatic bands scattered bilaterally.
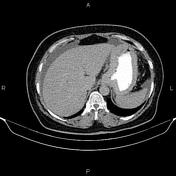
Increased wall thickness due to tumoral infiltration is present at gastric cardia and proximal of body; accompanied by perigastric fat stranding and a few small regional lymphadenopathies. In addition, mild to moderate abdominopelvic ascites and omental thickening are present.
An IUD is present within the uterine cavity in appropriate station.
Case Discussion
Path proven gastric adenocarcinoma with regional lymphadenopathies, abdominopelvic ascites and tumoral seeding.
CT is currently the staging modality of choice because it can help identify the primary tumor, assess for the local spread, and detect nodal involvement and distant metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.