
Presentation
Acute onset epigastric pain. No prodrome. Total white cell count > 15000.
Patient Data
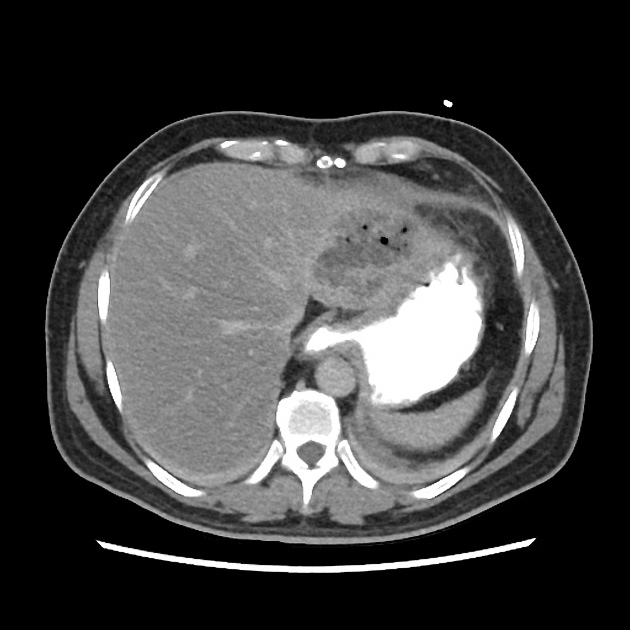
Fairly well defined poorly enhancing lesion with air foci within is seen in the left lobe of liver. Vessels seem to freely traverse the lesion.
No intra hepatic biliary dilatation, no other focal liver lesions. Normal opacification of hepatic vasculature.
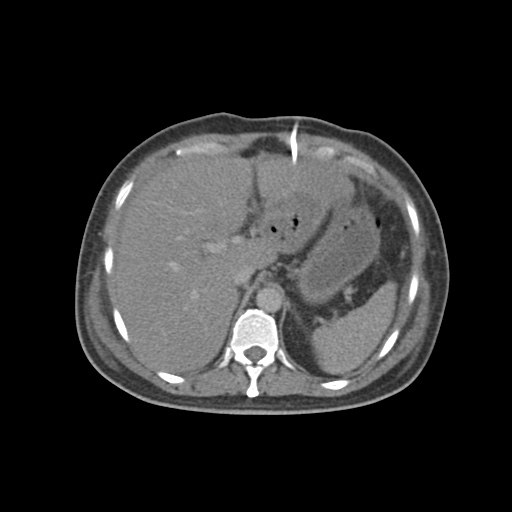
CT liver 48 hours after presentation & lesion drain tube insertion
Attempted pig tail for drainage did not provide any diagnostic or therapeutic relief.
Follow up CT just identified the drainage tube in situ in the lesion. Patient was clinically improving.


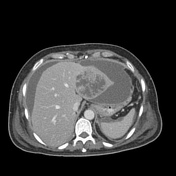

Day 10 CT with patient worsening clinically
Absence of air foci within lesion with the lesion appearing to be in a more liquefactive phase. However there is extensive wall enhancing ascitic fluid all around the liver extending inferiorly into the right paracolic gutter. Another pocket is also seen in the perisplenic and left paracolic gutter.
Case Discussion
This case in hand is a good demonstration of a hepatic abscess in evolution. The relatively solid hepatic lesion along with intravenous antibiotic therapy appeared liquefied in a week's time. Liver abscesses can breach the liver capsule and result in secondary spread of infection into the peritoneum as identified in the follow up CT.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.