
Presentation
Abdominal pain increasing in the last week.
Patient Data




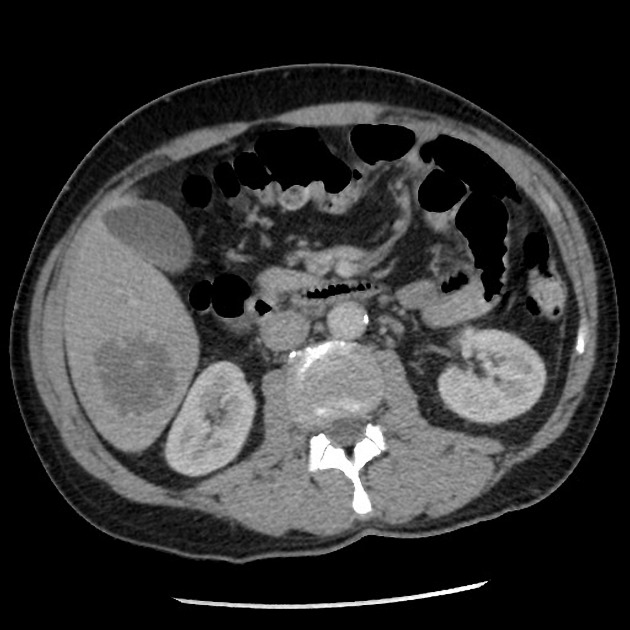
There is a segment VI hypodense mass lesion with an irregular thin rim of enhancement and appearances of internal crossing vessels. A few small hypodense liver lesions scattered in the right hepatic lobe are felt to represent cysts. Small amount of free fluid in the peritoneal cavity. The study is otherwise unremarkable.
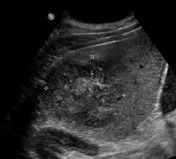
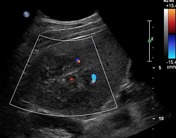


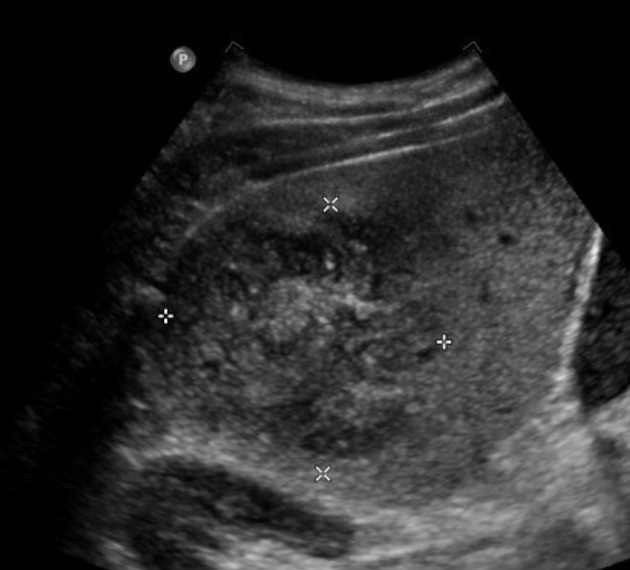
Targeted liver images confirm the segment VI lesion to have a heterogeneous content and internal vascularity.
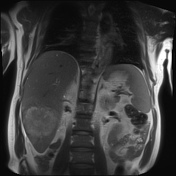
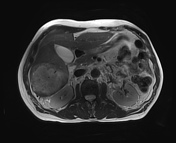
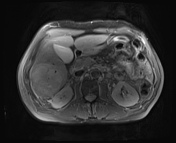
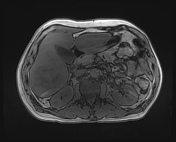
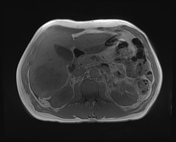
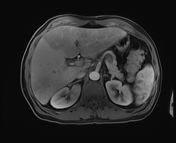
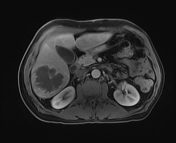
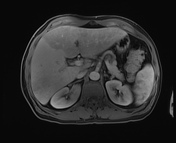
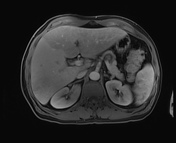
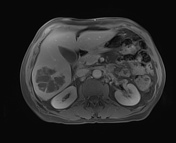
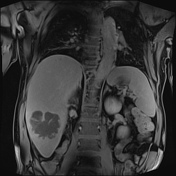
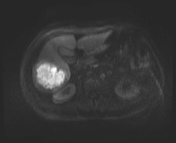
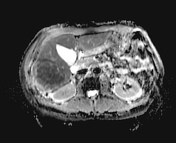

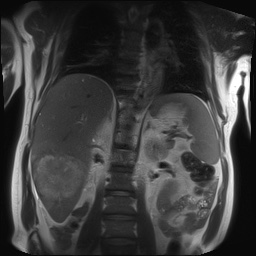
There has been increase in the size of the segment VI liver lesion since the last CT, showing features of an abscess and characterized by heterogeneous intermediate T2 signal, marked internal diffusion restriction, and thick irregular surrounding enhancement. It measures approximately 6.6 x 7.0 x 7.6 cm (volume 190 ml). The liver shows perfusional abnormalities involving the left lobe in the early post contrast phases, likely related to the inflammatory process, no signs of portal vein thrombosis noted. Also, there are features of periportal edema, particularly around the right portal tracts. Multiple small simple cysts scattered through the liver parenchyma. Small amount of free fluid adjacent to the liver capsule.
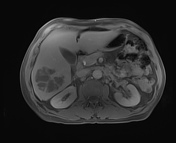
The gallbladder has sludge forming fluid-fluid level within, but no convincing inflammatory changes. There is no intra or extrahepatic biliary tree dilatation, no filling defects to suggest choledocholithiasis. The pancreas has normal appearances, the main pancreatic duct is not dilated. The adrenal glands, spleen, and kidneys are normal. No upper abdomen lymphadenopathy.
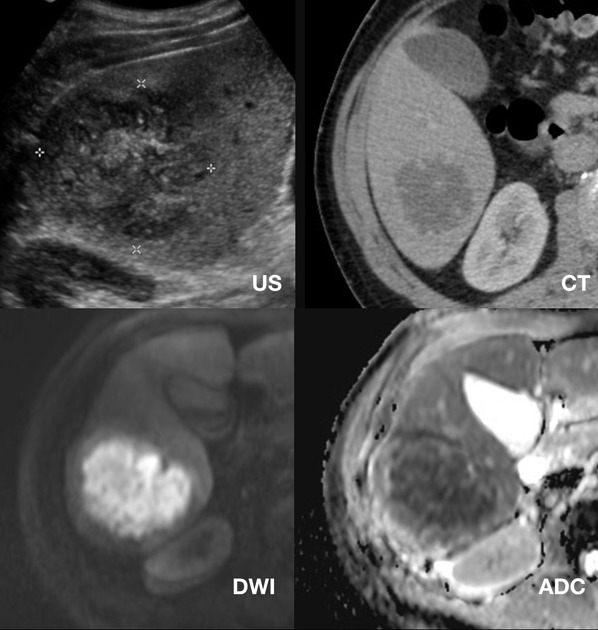
Side-by-side images of US, CT, and DWI/ADC MRI sequences.
Case Discussion
This case shows typical imaging features of a liver abscess that was misinterpreted on the first CT scan due to misleading clinical information and therefore, ended having an MRI with Primovist. The fact that the abscess encases a central vessel was interpreted as a possible FNH on the patient's portal venous CT. With the clinical picture of subacute RUQ pain and fevers, abscess easily comes into consideration. MRI features are characteristic for an abscess.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.