
Hepatic pseudolesion secondary to superior vena cava obstruction
Presentation
Shortness of breath, cough and weight loss. CXR shows right-sided mass. Staging CT.
Patient Data
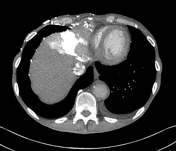






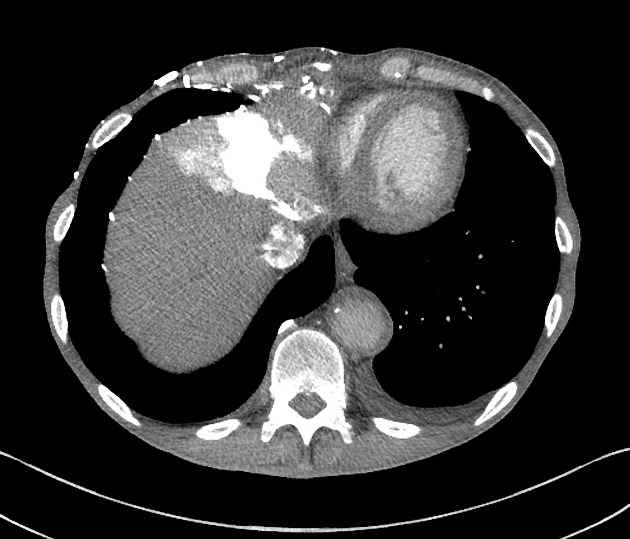
Large confluent right-sided mass invading into superior and central mediastinum. SVC compression. Right hilar adenopathy. Numerous collateral vessels opacified around right shoulder, and along right anterior chest wall. Dense blush of contrast opacification in segment IVa of the liver, with less dense opacification immediately lateral to this. Dense opacification of the inferior vena cava - more than is expected for the initial phase. Persistent abnormal density in liver on portal venous phase. Left adrenal nodule.
Case Discussion
The hepatic lesion is, in fact, a pseudolesion caused by abnormal contrast accumulation due to superior vena cava obstruction (SVCO) by a malignant and infiltrative mass. In SVCO, if contrast is injected into an upper limb vein, it is diverted into collateral pathways that ultimately direct the flow of blood (and therefore the contrast) into the IVC in order to reach the right side of the heart. These collateral pathways include the internal thoracic, superior epigastric and inferior epigastric veins, which communicate with paraumbilical veins in the anterior abdominal wall around the umbilicus. The superior and inferior veins of Sappey are the chief paraumbilical veins and carry the blood (and the contrast) to the left lobe of the liver, with direct hepatic parenchymal perfusion as well as drainage into branches of the portal vein. This dual drainage explains the two different densities observed within the area of avid enhancement.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.