
Presentation
Abdominal pain, fever, leukocytosis.
Patient Data




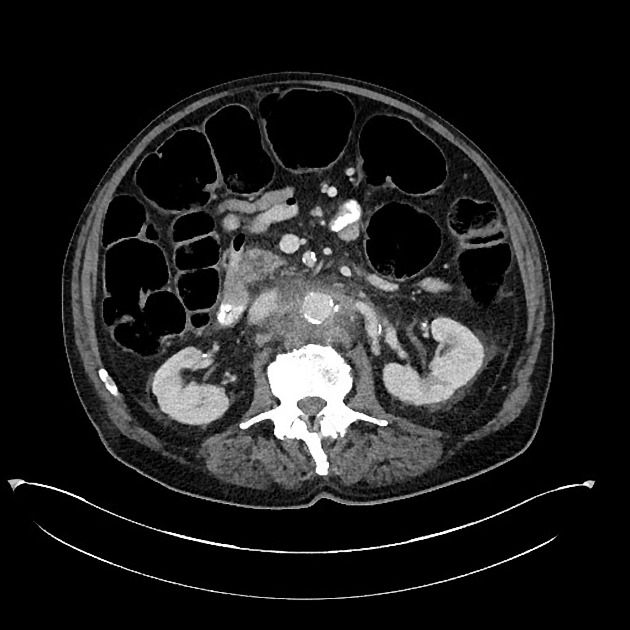
Heavy atherosclerosis of the abdominal aorta, mesenteric, and iliac vessels. Hazy stranding and mildly prominent lymph nodes about the abdominal aorta at the level of and slightly inferior to the renal arteries. No definite periaortic gas is identified. No aortoenteric fistula.
Posterior projecting small pseudoaneurysm at the level of the right renal artery, with the defect in the wall measuring 6-7 mm and the extraluminal collection measuring 2.1 x 0.8 x 1.2 cm. Focal ectasia measuring 2.6 cm in the mid segment of the infrarenal abdominal aorta
without aneurysm.
Severe narrowing and heavy plaque at the origin of the right renal artery. Ill-defined rounded area of low attenuation along the anterior interpolar cortex which could represent small area of inflammation, infarction, or mass.
Colonic dilation with large amount of stool.
Case Discussion
Laboratory values:
WBC 24k
Lactate 13
Blood cultures positive for MRSA
Infectious aortitis with small pseudoaneurysm. The periaortic stranding, adenopathy, and history of fever with leukocytosis should lead to very high suspicion for this diagnosis. The pseudoaneurysm is likely mycotic in origin.
Attempt at cadaveric repair was unsuccessful due to irreversible coagulopathy, eventually resulting in the patient's demise.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.