
Presentation
Progressive difficulty mobilization. Prior laminectomy. Currently wheelchair bound.
Patient Data



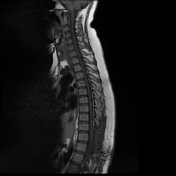
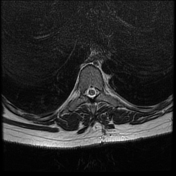
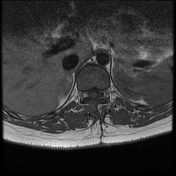

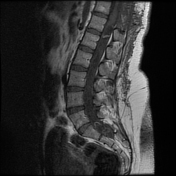
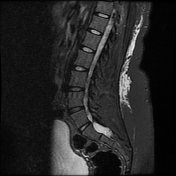
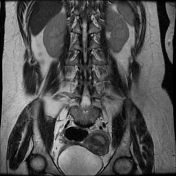

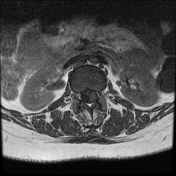
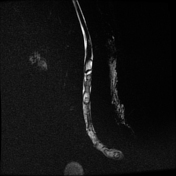

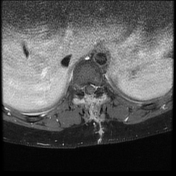
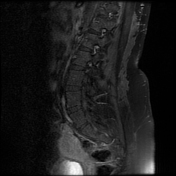
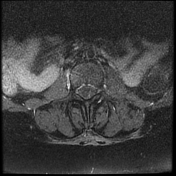
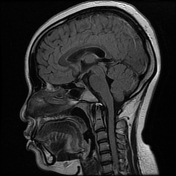
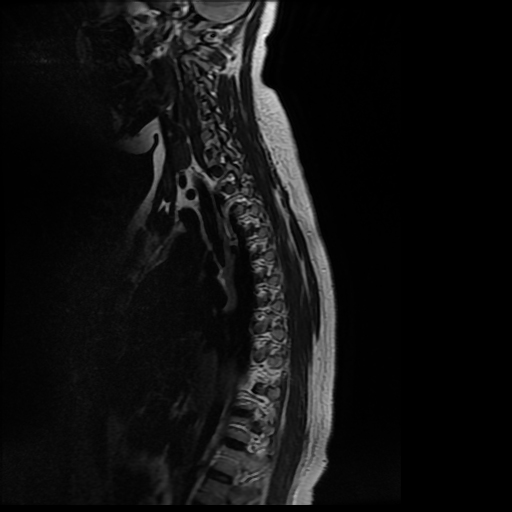
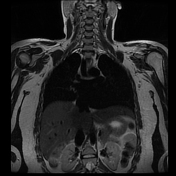
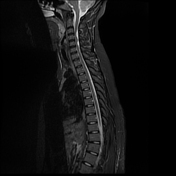
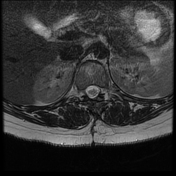
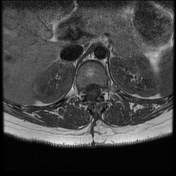
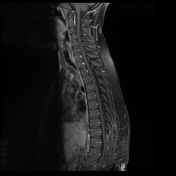
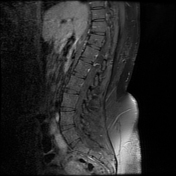
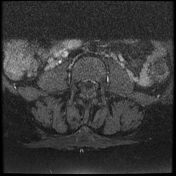
Multilevel extramedullary intradural/intrathecal cystic lesions scattered in the entire spinal canal but predominantly in the lumbar region, demonstrated high signal intensity on T2/STIR and some of the cystic lesions demonstrated T1 rim hyperintensity and high signal intensity changes in the conus medullaris probably from mass effect or inflammatory response.
Soft tissue enhancement with an abutment to the dorsal aspect of the spinal canal with posterior element changes most likely postoperative changes.




After six months on albendazole treatment, the patient showed significant clinical improvement with no significant changes in imaging findings.
Case Discussion
The differential considerations of the above findings in the absence of histopathology are spinal neurocysticercosis, diffuse arachnoiditis due to persistent infection with fungal/atypical organism with intrathecal adhesions at the lumbosacral region, and multifocal cystic peripheral nerve sheath tumor.
Given the above differential diagnosis, T9-T10 laminectomy was done for biopsy (the soft tissue enhancement seen in the first set of images) and histopathology results revealed Taenia solium (pork tapeworm) infection.
The patient was put on albendazole for six months and at the time of the follow-up MRI examination, she was able to walk without significant assistance.
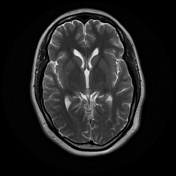
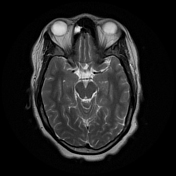
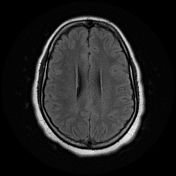
Isolated spinal neurocysticercosis is a very rare disease entity with few reported cases in the literature. In spinal neurocysticercosis, often there is concomitant intracranial involvement, which was absent in this case.
Post treatment radiological changes are mainly dependent of the pretreatment stage of the disease.
Neurocysticercosis is commonly encountered in southern Africa region including Botswana even though data on the actual prevalence of taeniosis and neurocysticercosis is lacking for Botswana1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.