
Presentation
Abdominal pain and vomiting. Midline abdominal mass feeling on physical exam.
Patient Data


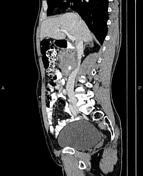

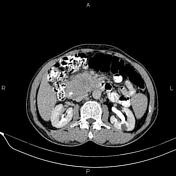
Asymmetrical increased wall thickness due to tumoral infiltration is present in the second and third parts of the duodenum that infiltrate the adjacent pancreatic head and cause duodenal luminal narrowing. The mass compresses IVC and displaces the mesenteric vessels without invasion or encasement. The pancreatic duct is not dilated.
A few prominent lymph nodes are seen in the vicinity of the mass.
A 25mm ill-defined low-enhancing mass-like lesion is noted in the 6th hepatic segment. In addition, two small masses, 15mm and 7mm, are observed in the 7th segment. All of the mentioned lesions become isodense with surrounding parenchyma on delayed images.
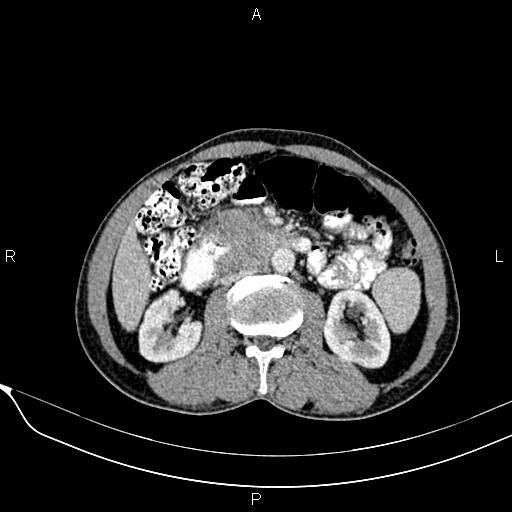
A few small non-enhanced simple cortical cysts are seen in both kidneys. Two small stones less than 5mm are also seen in the upper calyces of the right kidney.
The prostate gland is enlarged.
Case Discussion
Histopathology and IHC proven duodenal adenocarcinoma with involvement of the pancreatic head.
Most of the masses that involve both pancreatic head and duodenum are pancreatic cancers, and duodenal adenocarcinoma is less common.
Although duodenal adenocarcinoma is the most common primary malignancy of the duodenum but represents only 0.3% of all gastrointestinal malignancies. More than 50% of duodenal adenocarcinomas have metastases at the time of diagnosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.