

Presentation
Premature birth. Day 6 portable chest and abdominal X-ray.
Patient Data
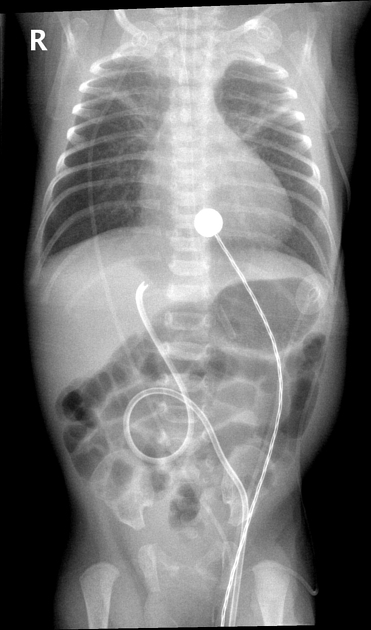
Hyperinflated lung fields with a central trachea and a normal cardiothoracic ratio. The ET tube is poorly identified, however, the tip is at the inferior margin of the T2 vertebral body, infraclavicular and satisfactorily sited. The nasogastric tube is satisfactorily sited. There are overlying ECG leads and a temperature lead.
The umbilical venous catheter (UVC) is malpositioned and likely within the proximal left portal vein. There are no suspicious intrahepatic lucencies.
There is a moderately severe surfactant deficiency disorder with hemo- or pneumothoraces.
The bowel gas pattern is smooth, with no other features suggesting necrotizing enterocolitis (NEC).
There are 12 pairs of ribs.

Features consistent with an acute intrahepatic fluid collection measuring 12.4 x 7.5 x 9.8 mm in diameter. This is demonstrated by a homogenous, echogenic, mass-like, irregular lesion within the right lobe of the liver.
There is no associated portal venous thrombosis and no intralesional gaseous lucencies.



The follow-up ultrasound 2 days later confirms a resolving acute intrahepatic fluid collection. It remains echogenic, and homogeneous, with the continued absence of any associated gaseous locules. The portal vein is patent and normal. The UVC has been removed and is not identified on the follow-up ultrasound.
Case Discussion
Features consistent with an acute intrahepatic fluid collection (TPNoma) due to the confirmed infusion of hypertonic fluid and TPN via a malpositioned UVC 1. Acute UVC-related intrahepatic fluid collections are homogeneous, echogenic and have a mass-like appearance 1.
The UVC was removed and replaced subsequently with a Broviac line given the ultrasound findings.
The smooth bowel gaseous pattern preceded a confirmed NEC a few days later.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.