
Presentation
Abdominal pain with vomiting three days after eating clam chowder. White blood cell count was 32.000 U/μL, with neutrophilia (90%); other blood tests were in normal range. Body temperature was 39.2°C.
Patient Data


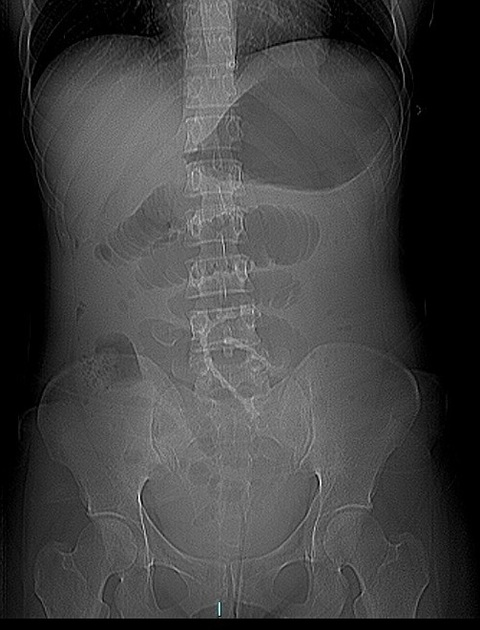
There are multiple dilated jejunal loops in the upper and middle abdomen. There is no air in the rectosigmoid. In the right iliac fossa there is a clam shell of about 2 cm.
Abdomen with contrast






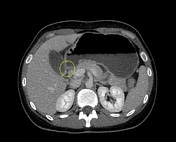
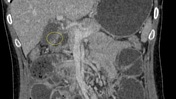
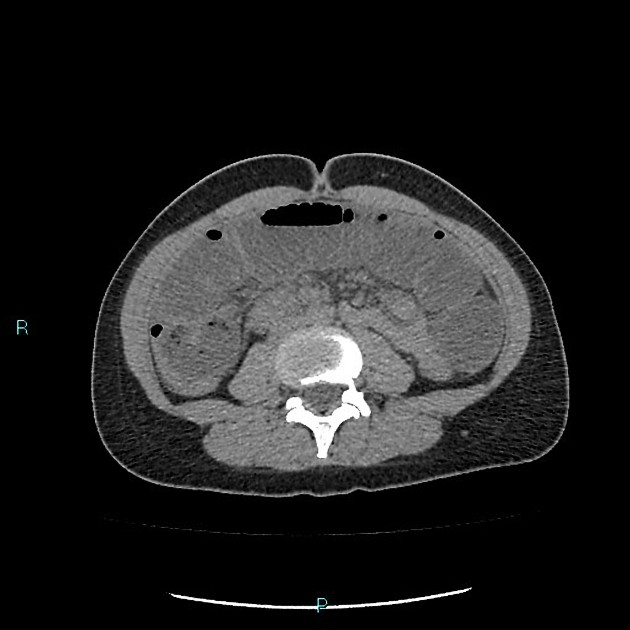
CT scan shows mechanical bowel obstruction caused by clam shell at the distal ileum with pneumoperitoneum and peritoneal effusion by bowel perforation. The small bowel feces sign and dilated proximal bowel loops are also identified. Left ovary enlarged.
Immediate laparotomy revealed the shell in the distal small bowel.
Resection of the last ileal loop and cecum with ileo-colic isoperistaltic anastomosis.
Case Discussion
Initial abdominal plain radiograph should be obtained when foreign body ingestion is suspected, which differentiates a radiopaque from radiolucent foreign bodies. Computed tomography with 3D reconstruction (3D-CT) is recommended with radiolucent foreign bodies. The presence of intestinal obstruction necessitates surgical intervention to extract the ingested foreign body.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.