
Megaureters due to bilateral duplex kidneys (prenatal and neonatal imaging)
Presentation
First pregnancy ultrasound performed at 20 weeks gestation. Standard risk pregnancy. No relevant familial history.
Patient Data
Prenatal US at 26WG

Bilateral megaloureters followed all the way from the renal pelvis to below the bladder. The bladder is identified thanks to the umbilical arteries at its borders drawing a Y-shape. Female fetus.
Prenatal MRI at 28WG


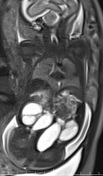
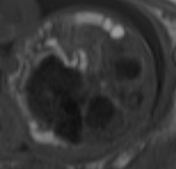
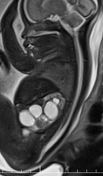
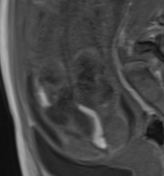
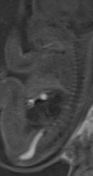
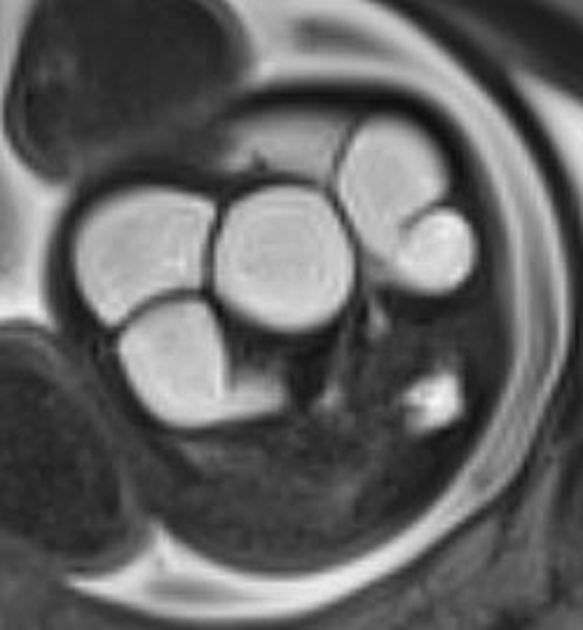
Bilateral megaureters as seen on US. The most important findings of MRI are:
- well-defined bladder within pelvic area (no extrophy)
- normal meconial filling of the colon with physiological rectal pouch
- normal spinal cord and no sign of sacral defect
- no obvious hydrometrocolpos
These findings are important to rule out associated malformations in the spectrum of a persistent cloaca in a female fetus.
A sharp eye may witness a separate pyelix at the lower pole of the right kindney on the coronal T2w image.
Prenatal US at 31WG
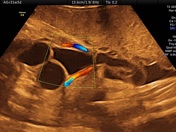


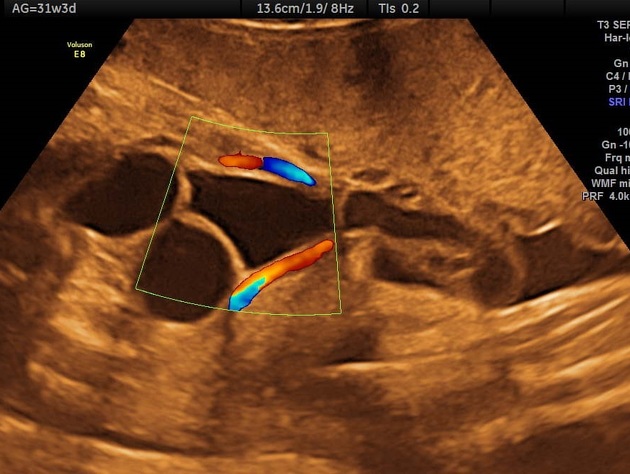
Stable findings at 31WG:
Bilateral megaloureters followed all the way from the renal pelvis to below the bladder. Bladder is identified thanks to the umbilical arteries at its borders drawing a Y shape. Bladder does not appear distended, no internal image of ureterocele.
Enlarged kidneys, with normal parenchyma: no thinning, no hyperechoic aspect.
A sharp eye may witness a separate pyelix at the lower pole of the right kindney on the axial US scan.
Oddly, calyces are non dilated and amniotic fluid remains normal, while oligohydramnios/anamnios might be expected in urinary obstacles.
Careful US examination reveals normal small bowel. The transverse large bowel is clearly seen, normal, non dilated. Fetal anal sphincter is normal (not shown).
Neonatal US




Duplex pelvis, with dilation of the superior pelvis and ureters on both kidneys. Normal bladder. Normal uterus anatomy.
Case Discussion
This is a case of megaureters in a female fetus. The most important differential diagnosis to rule out in such clinical context in prenatal diagnosis is a persistent cloaca, for it bears a poor prognosis (severe perineal malformation with bladder exstrophy and a common urogenitorectal sinus with or without sacral and spinal cord defects). The detailed US is critical, and MRI has a significant plus-value to assess the meconial physiological colon filling and spine cord examination. In this case, cloaca has been ruled out.
The bladder remained normally filled, non-distended: this is not a case of lower urinary tract obstruction (LUTO) (i.e below bladder obstacle), but rather a case of bilateral lower ureter obstacle or ectopic insertion. On strict axial scan, the ureteral end-pouches were seen lower than the bladder. The uterus was not seen on prenatal imaging (no obvious hydrometrocolpos). The amniotic fluid remained oddly normal throughout pregnancy, indicating normal diuresis.
The bilateral kidney duplex system was not properly identified on prenatal imaging: it has been diagnosed on the neonatal US. However, normal amniotic fluid and normal blood creatinine levels at day 3 are easily explained by the duplex collecting system and are additional clues leading to right diagnosis. Moreover, with a retrospective examination, a lower normal pyelix could be seen on both US and MRI on the right side. Still very hard to see on the left.
Dr F Cuillier and Dr M Balu also significantly contributed to this case.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.