
Presentation
History of epilepsy and cirrhosis, presenting with sudden-onset dysarthria.
Patient Data
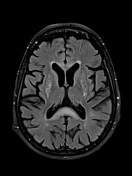

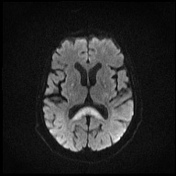
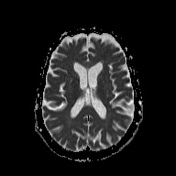
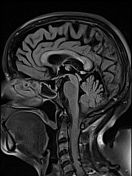

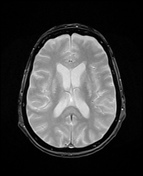
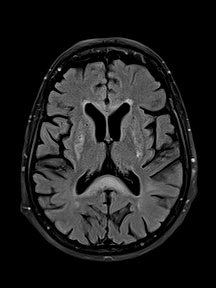
Bilateral symmetric T2 and FLAIR hyperintense lesions are seen in the dentate nuclei of the cerebellum, the corpus callosum, and subcortical frontal white matter.
DWI shows mild hyperintensity of the splenium of the corpus callosum and dentate nuclei without restriction on the ADC map.
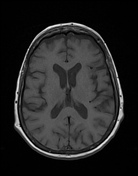
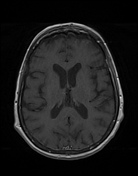
No detectable enhancement of the lesions.
Mild diffuse cerebral atrophy.
Bilateral mastoiditis.
Case Discussion
After questioning, it turned out that our patient had been taking metronidazole for the past 20 days.
Metronidazole, an antibiotic commonly used to treat various infections, has been associated with potential neurotoxicity affecting the central nervous system (CNS), especially with prolonged or high-dose use.
Metronidazole-induced encephalopathy is characterized by altered mental status, cerebellar dysfunction, and sometimes reversible brain lesions observed on MRI, typically in the cerebellum, brainstem, or corpus callosum.
Discontinuation of the drug often leads to a gradual resolution of symptoms as in our case, highlighting the importance of recognizing these adverse effects early in patients presenting with unexplained neurological signs while on metronidazole therapy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.