
Presentation
History of cerebral vascular accident. ECG showed atrial fibrillation.
Patient Data






Left ventricle:
normal sized chamber with normal left ventricular wall thickness
no thrombus
borderline systolic function LVEF: ~50-55%
Right ventricle:
mildly dilated, basal diameter: ~4.1cm with borderline systolic function
TAPSE: 1.6 cm
tissue Doppler imaging systolic velocity (TDI S'): 10 cm/s
Interventricular septum: intact
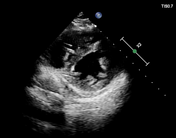
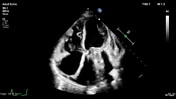
Atria:
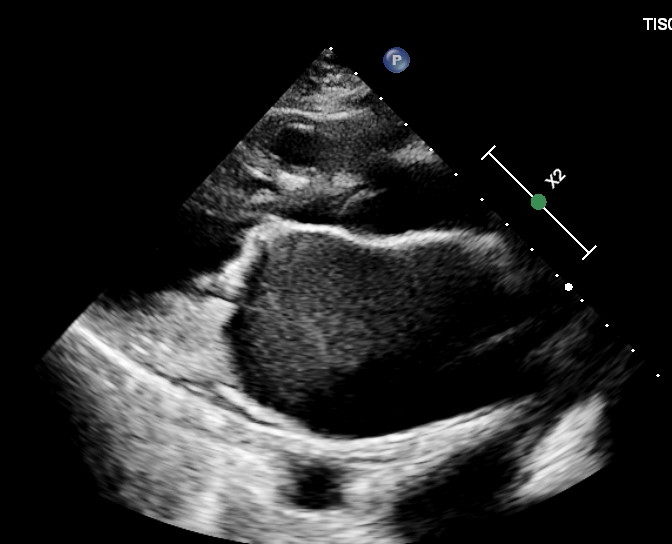
left atrium: dilated, area: 41 cm2, LAVI: 84 mL/m2 with smoke appearance within the chamber (spontaneous echo contrast)
right atrium: dilated, area: 27 cm2
Aortic valve:
normal tricuspid
no aortic regurgitation
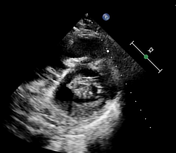
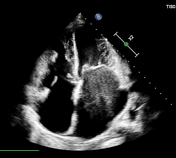
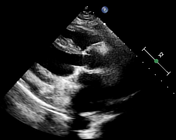
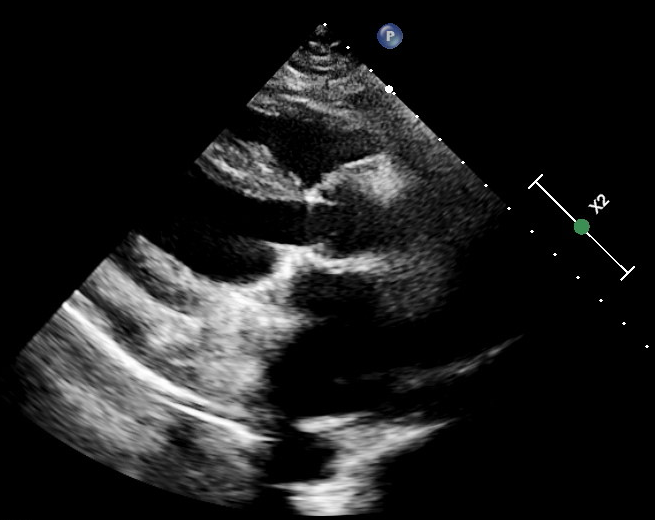
Mitral valve:
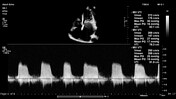
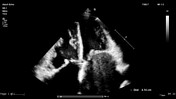
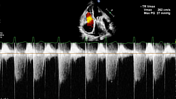
thickened and calcified mitral valve leaflet tips with diastolic doming of the anterior mitral valve leaflet giving a "hockey stick" appearance and restricted motion of the posterior mitral valve leaflet. No mitral regurgitation
mitral valve area by PHT: 0.30 cm2, transmitral mean pressure gradient: 17 mmHg
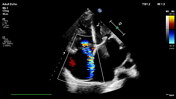
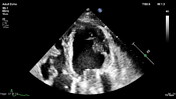
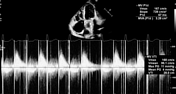
Tricuspid valve:
severe eccentric tricuspid regurgitation
Additional findings:
severely elevated pulmonary pressures (estimated sPAP ~80 mmHg)
dilated IVC with <50% inspirational collapse, dilated hepatic veins
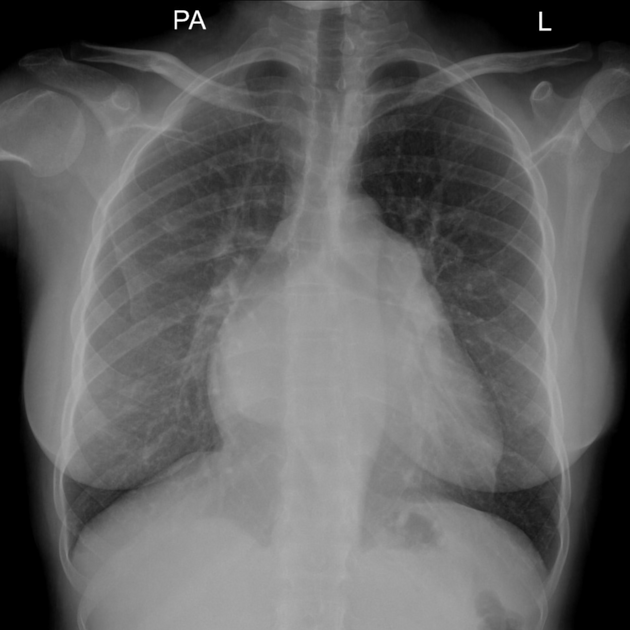
The heart is enlarged CTR 15:26. Enlarged left atrium is seen splaying the carina.
Filling of the pulmonary bay is noted. No hilar or mediastinal adenopathy is seen.
Lungs show normal aeration. Costophrenic and cardiophrenic angles are clear. Bony cage appears intact.

Post mitral valve replacement
mechanical prosthetic mitral valve is normally functioning. No mitral regurgitation. No paravalvular prosthetic leaks noted
mitral valve area by PHT: 3.28 cm2, transmitral mean pressure gradient: 4 mmHg, mitral valve PHT: 67 ms
-
no pulmonary arterial hypertension estimated sPAP ~32 mmHg)
Case Discussion
This is a case of severe mitral valve stenosis due to rheumatic heart disease. The patient was scheduled for surgery which was successful.
Echocardiography is the primary imaging method for assessing prosthetic valve performance and diagnosing prosthetic valve failure.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.