
Presentation
Sepsis and chest pain
Patient Data
Age: 20 years
Gender: Male
From the case:
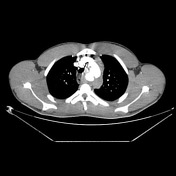
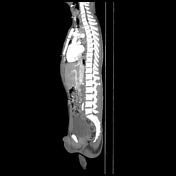
Mycotic aortic aneurysm



Download
Info

Two saccular aneurysmal dilations arise from the aortic arch, the largest 2.5 cm, associated with an adjacent mediastinal hypodense collection with peripheral contrast enhancement.
Case Discussion
Mycotic aneurysms generally result from systematic bacterial infections, mostly of cardiac origin. In this case, we see how the aortic arch is involved with an associated mediastinal collection of which Staphylococcus aureus was identified as the causative agent. Complications related to this pathology are the rupture of aneurysms and persistent sepsis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.