
Presentation
History of left leg trauma (fall) 6 months ago, followed by mild pain in left distal leg. Known case of sickle cell disease.
Patient Data



A well-defined eccentric, multi-septated radiolucent lesion with a narrow zone of transition and sclerotic margins is noted in the left distal femoral metaphysis. Mild endosteal scalloping is noted. No internal chondroid/ossific matrix, periosteal reaction, obvious fracture, or associated soft tissue abnormality is appreciable.
Based on the radiographic features, the differential diagnosis includes an aneurysmal bone cyst (ABC), fibrous dysplasia, or giant cell tumor (GCT) of bone.
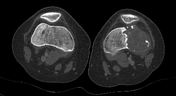




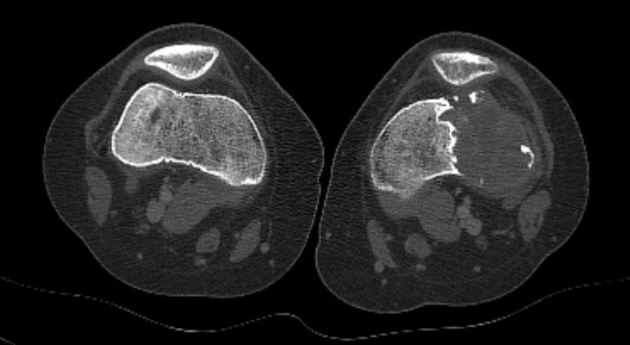
CT shows an eccentric purely radiolucent lesion in the distal femoral meta-epiphyseal region. It has a well-defined sclerotic medial border, narrow zone of transition, and mild periosteal reaction. Cortical breakthrough is noted along the anterior, posterior, and lateral aspects.
Based on the CT finding, the preferred imaging diagnosis of GCT was made.
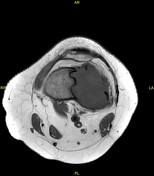
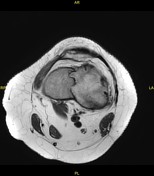

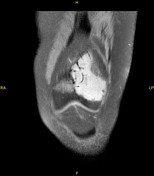
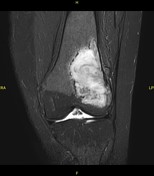
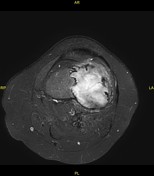
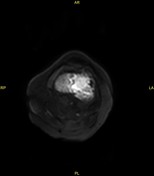
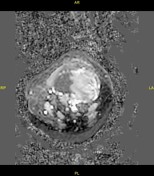
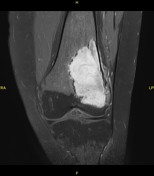

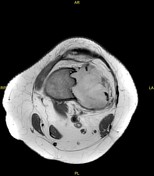
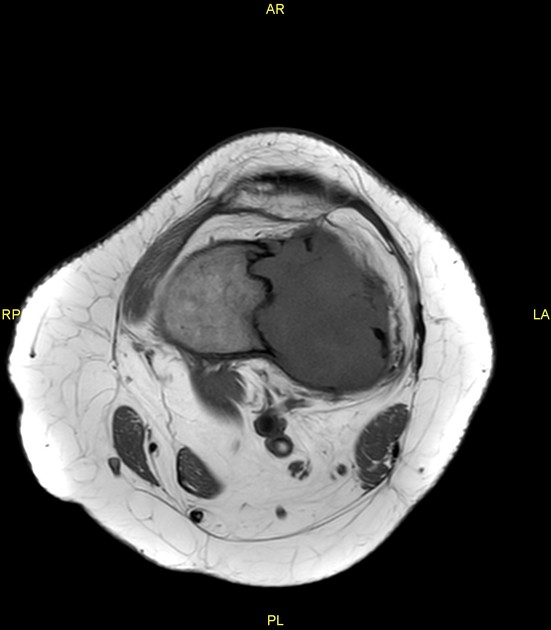
There is a focal lobulated space occupying lesion in distal metaphysis of left femur. The lesion is hyper intense on T2, STIR and fat-suppressed T1-weighted; and iso- to hypo-intense on T1-weighted images with moderate contrast enhancement on post contrast images. The lesion does not show abnormal restriction on DWI. It has peripheral low signal intensity rim (corresponding to radiographic sclerosis) along its medial aspect and has multiple small focal internal hypo-intense areas (fibrosis/sclerosis?). Cortical interruption is noted along the anteroposterior and lateral aspects of the lesion; however, no significant extra-osseous soft tissue component is seen. No hemorrhage, necrosis, or fluid-fluid levels are noted in the lesion.
After the MRI, the differential diagnosis was widened to include atypical GCT, fibrous dysplasia, ABC or chondromyxoid fibroma.
The patient underwent surgery. A fibrous lesion was found in the left distal femur, which was curetted, and a diagnosis of non-ossifying fibroma was made on histopathology.



Postoperative radiograph:- Lesion was curetted and the defect was filled with bone cement & graft. Internal fixation of the left distal femur with a metallic plate & screws was also done.
Case Discussion
Non-ossifying fibromas are the commonest non-neoplastic fibrous osseous lesions, usually seen in the metaphyses of long bones of young patients with immature skeletons 1,2. Most of the patients are asymptomatic, and it is commonly discovered as an incidental finding on plain radiographs done for some other purpose; however, a few patients (with larger lesions and/or pathological fractures) can present with pain and swelling 1,2. Most of these lesions are seen in the long bones of the lower extremities, especially around the knee (distal femur and proximal tibia) 2. Herget et al. reported 79% lesions around the knee 2. Because of increased risk of fracture, all non-fibular lower limb lesions > 33 mm in the vertical length and affecting > 50 % of the bone diameter in both planes (lateral & anterior-posterior), need close monitoring 2. Because of the high incidence of spontaneous healing in most cases, most large NOFs can be conservatively managed 2.
NOF has a classical imaging feature on plain radiography (well-marginated, eccentric, intramedullary radiolucent lesion with dense sclerotic margins towards the medulla, aligned along the long axis of the bone, etc.) 1,2. However, its MR imaging features fluctuate and depend on the relative combinations of the fibrous tissue, collagen, foamy histiocytes, hemorrhage, and bone trabeculae (depending on the development or healing phase of the lesion) 3.
Aneurysmal bone cyst, chondromyxoid fibroma, intraosseous ganglion, and fibrous dysplasia are the major imaging differential diagnoses 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.