Presentation
Seizure
Patient Data


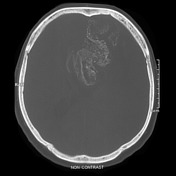

Selected single images from a CT demonstrate a large left frontal lobe mass with prominent gyriform calcification. It appears to extend across the corpus callosum.
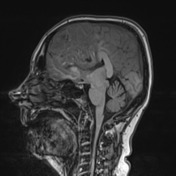

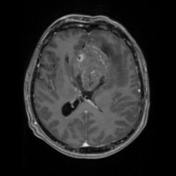
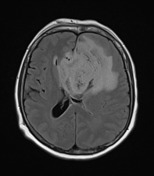
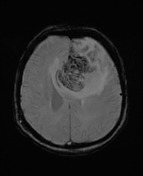
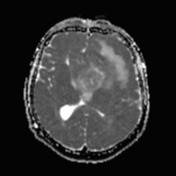
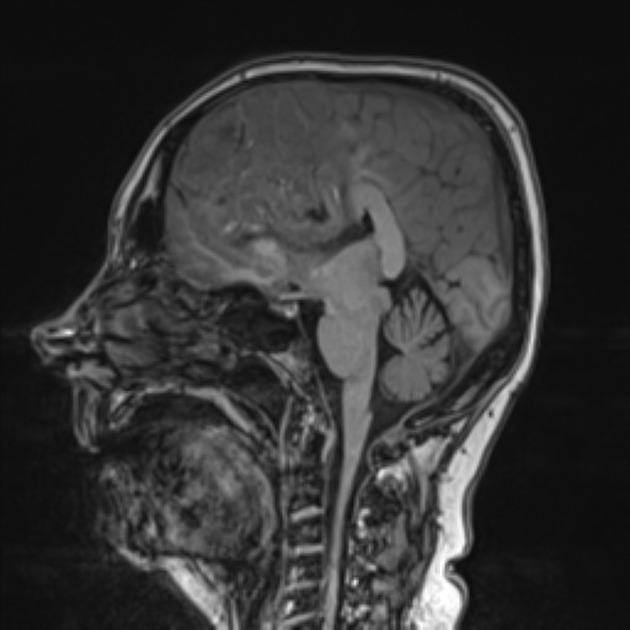
There is extensive FLAIR abnormality within the left frontal lobe with prominent cortical involvement with thickening. The FLAIR signal abnormality extends across the genu of the corpus callosum into the right frontal lobe. A relatively small region of FLAIR suppression is demonstrated centrally within the frontal lobe white matter FLAIR hyperintensity. There is patchy contrast enhancement. Extensive gyriform susceptibility induced signal dropout is demonstrated, with cortical T1 hyperintensity, corresponding to gyriform calcification demonstrated on CT.
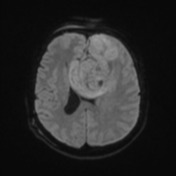
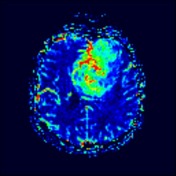
There is marked elevation of CBV. Intermediate (facilitated compared to normal brain) diffusion restriction. MRS (not shown) demonstrates elevated choline, reduced NAA and a lactate peak.
There is a large amount of mass effect, with effacement of the left lateral ventricle and frontal horn/body of the right lateral ventricle and 2cm rightward midline shift. There is mild dilatation of the right lateral ventricle temporal horn and FLAIR hyperintensity surrounding the body of the right lateral ventricle, consistent with transependymal fluid shift.
Scattered foci of FLAIR hyperintensity within the right frontal and left parietal lobes are more prominent than expected for age, however likely relate to chronic small vessel ischemic change.
Conclusion:
Findings are most consistent with a left frontal high-grade glial series tumor. Prominent calcification suggests oligodendroglial component.
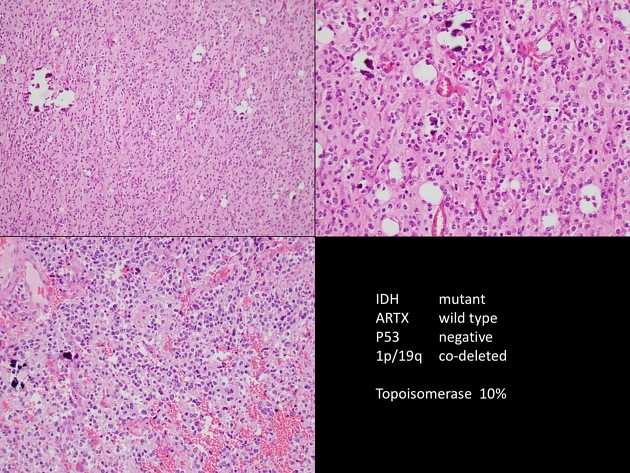
Sections show a hypercellular tumor composed of moderately pleomorphic cells containing round to oval, hyperchromatic, vesicular nuclei with inconspicuous nucleoli and prominent perinuclear clearing. Tumor cells are arranged in diffuse sheets intersected by thin-walled "chicken-wire" capillaries. Abundant tumor microcalcification is present. No necrosis or microvascular proliferation is seen. Extracellular non-refractile foreign material and hemorrhage are present, consistent with recent surgery.
- IDH-1 R132H mutation: positive
- 1p19q: co-deleted
FINAL DIAGNOSIS: oligodendroglioma (WHO Grade II).
Case Discussion
Although not seen as frequently as older textbooks would suggest, prominent calcification, particularly of a mass with significant cortical expansion, is a typical appearance of an oligodendroglioma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.