
Presentation
A patient presented with upper abdominal pain. His laboratory profile showed an elevated Lipase of 22,000 units. There was a prior history of acute pancreatitis, one year before, which resolved without complications. No history of gallstones or alcoholism
Patient Data
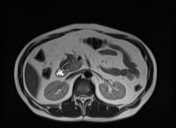



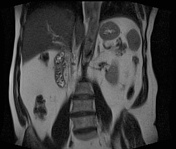

Large dorsal pancreatic duct measuring 3 mm in diameter and opening into minor papilla along the medial border of second part of the duodenum.
A smaller ventral duct measuring 1.5 mm in the pancreatic head is seen which joins distal common bile duct, to open into major papilla along the second part of the duodenum . A small branch from ventral duct also joins dorsal duct.
CBD is normal and measures 4 mm in diameter. Gallbladder and cystic duct are normal. Intrahepatic biliary radicles are normal. Pancreas appears normal. No intraductal filling defects or cystic lesions are noted.
These findings favor a diagnosis of pancreas divisum.
Case Discussion
A non-alcoholic patient with no evidence of gallstones presented with a second episode of abdominal pain and clinicopathological diagnosis of acute pancreatitis. MRCP was requested by the clinician with suspicion of pancreas divisum in this case of idiopathic pancreatitis.
MRCP shows a large dorsal duct draining the pancreas and opening into minor papilla along the medial border of second part of the duodenum. A small ventral duct is seen in the pancreatic head which joins the distal CBD to then open into major papilla along the medial border of second part of the duodenum. A small branch from ventral duct also joins the dorsal duct. No evidence of any cyst or filling defects related to ducts is seen. Pancreas divisum is a developmental anomaly with partial or complete failure of fusion of dorsal and ventral buds.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.