
Presentation
The patient started to complain of diffuse abdominal pain as well as a tense tender bulge adjacent to the stoma opening.
Patient Data
Age: 40 years
Gender: Male
From the case:
Parastomal hernia


Download
Info

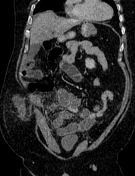
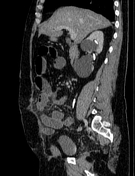
There is a cluster of small bowel loops and bowel mesentery protruding through the abdominal wall muscles adjacent to stoma associated with free fluid and fatty stranding.
Proximal abnormally dilated and fluid-filled small bowel loops with mesenteric fatty stranding.
Bilateral renal cysts are noted.
The colon is non-visualized due to the previous total colectomy.
Case Discussion
Parastomal hernia considered the most common occurred long-term stoma complication with incidence reaches 50% 1.
In the above case, it leads to small bowel obstruction.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.