
Presentation
Generalized tonic-clonic seizure for one episode post-meal. Glasgow coma scale 6, intubated - reduced power over left limbs.
Patient Data


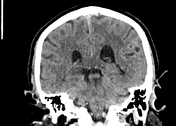

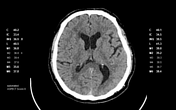
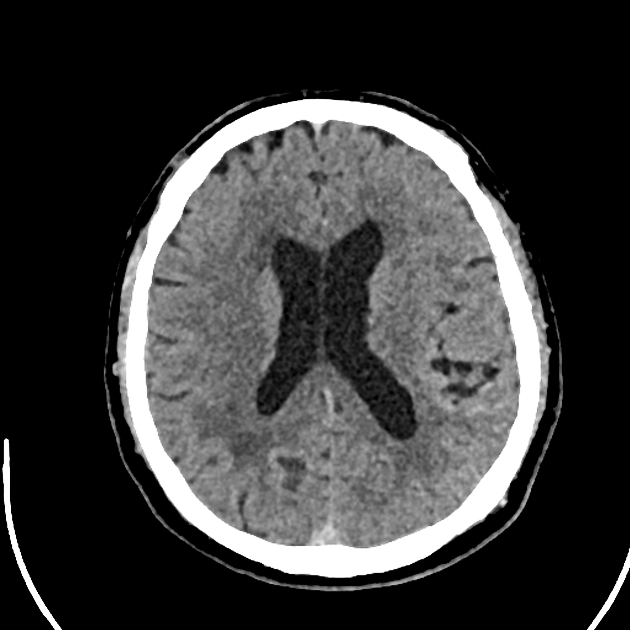
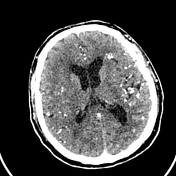
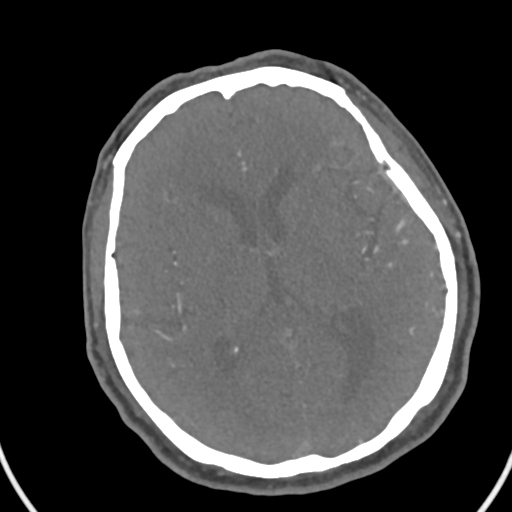
No acute intracranial bleed.
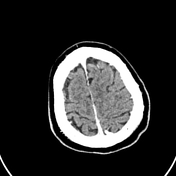
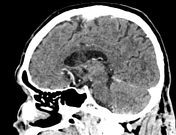
Hyperdense, tortuous cortical vessels with redundant sulci at the left parietal lobe.
No midline shift.
Ventricles, basal cisterns, and sulci are normal.
No skull vault lesion.
Features are suggestive of left parietal arterio-venous malformation. CTA and CTV Brain were suggested.
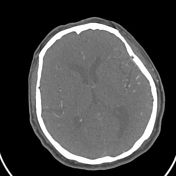
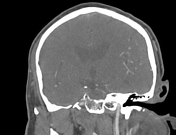
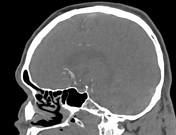


Abnormal serpiginous vessels at the left frontoparieto-occipital lobes and left cerebellum. These areas are supplied by the left MCA (middle cerebral artery) and left branches of the left ECA (external carotid artery) – left superficial temporal and left occipital arteries. Early draining veins, going into the left sigmoid, left transverse sinuses and superior sagittal sinus.
Aneurysmal dilatation at the left occipital temporal lobe, just superior to the left sigmoid sinus, but not within the sigmoid sinus.
Bilateral ICAs (internal carotid arteries), MCAs, ACAs (anterior cerebral arteries), and ACom (anterior communicating arteries) are well opacified.
Left PCom (posterior communicating artery) is not visualized.
Right, PCom is hypoplastic.
Bilateral vertebral, basilar, bilateral PCAs (posterior cerebral arteries), bilateral AICAs (anterior inferior cerebral arteries) and SCAs (superior cerebral arteries) are well-opacified.
Bilateral PICAs (posterior inferior cerebral arteries) are not visualized.
All the dural venous sinuses are patent.
No filling defect is seen within the sinuses.
Case Discussion
The radiological diagnosis is left frontoparietal-occipital lobes and left cerebellum arterio-venous malformation with flow-related aneurysms and possible dural arterio-venous fistula components.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.