
Presentation
History of right pelvic resection, now with thrombocytopaenia and acute kidney injury. The patient had a non-targeted left renal biopsy. Increasing flank pain and abdominal distention prompted a CT scan.
Patient Data




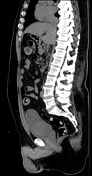

On the abdominal scout film there is a paucity of bowel gas in the left hemiabdomen.
There is a large hematoma in the left perirenal space, extending into the anterior and posterior pararenal spaces, as well as a small amount extending into the intraperitoneal space. The left kidney is displaced anteriorly.
The higher attenuation material represents more acute blood products. There is no discrete sentinel clot.
There is also a large rounded filling defect in the pelvis, compatible with a large clot in the bladder.
Case Discussion
Hemorrhage and hematoma are a risk in percutaneous renal biopsy, even if the patient has no specific risk factors. Small hematomas are common (~90% in one series), but large hematomas are uncommon.
Blood products in the abdomen start at blood pool attenuation. Then, as they age and the hemoglobin concentrates, the hematoma increases in attenuation (up to 60-80 HU). As the hematoma ages and becomes a seroma, the attenuation drops back to around 30 HU.
If the cause of a renal/perirenal hematoma is known (such as biopsy), then further imaging is not necessary unless the patient is not clinically improving and there is concern for an expanding hematoma. If the patient does not have a reason for the hematoma, then one should be concerned about an underlying mass that is hemorrhaging. The patient should return after resolution of the hemorrhage to assess for an underlying mass with contrast enhanced CT or MRI.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.