
Presentation
Known NSCLC with mediastinal infiltration with suspicious esophageal fistulation.
Patient Data
Age: 45 years old
Gender: Male
From the case:
Pneumomediastinum


Download
Info
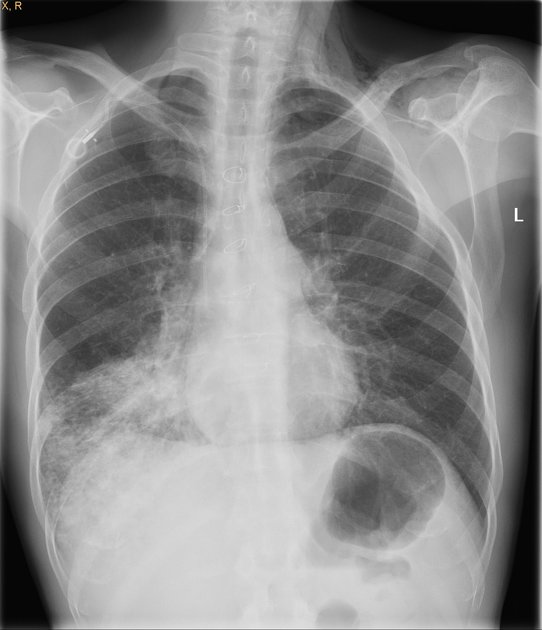
Right lower basal opacity representing the known lung tumor and distal collapse/consolidation. There is fine lucency along the inferior aspect of the cardiac shadow (continuous diaphragm sign) and linear air lucencies along the left side of the mediastinum representing pneumomediastinum tracking up to cause surgical emphysema in the left supraclavicular area.
Right sided portocath.
From the case:
Pneumomediastinum
Download
Info
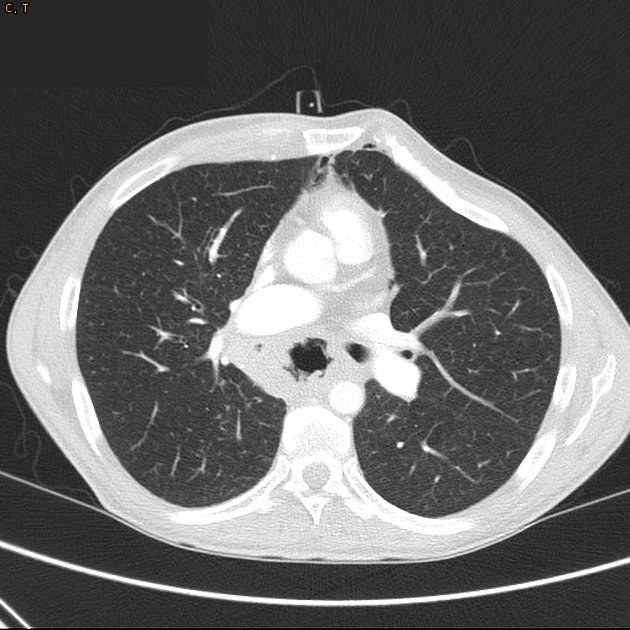
Right basal and medial infiltrative lung tumor. Surrounding tree-in-bud and reticulonodular lung opacities represent further lung infiltration. Mediastinal and esophageal invasion with esophageal-pulmonary fistulation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.