
Presentation
Transfer from DGH to neurosurgical center. Presented with few weeks of headache and reduced appetite. Worsening positional headache and new vomiting and dizziness. On examination, moderate cerebellar dysfunction (ataxia, poor alternating movements, dysdiadochokinesis).
Patient Data




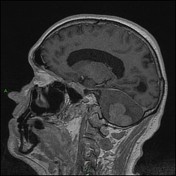
Large hyperdense and enhancing left cerebellar mass with local surrounding edema. Left inner table bony defect representing either a cerebellar encephalocele or venous lake. No history of surgery or regional trauma.
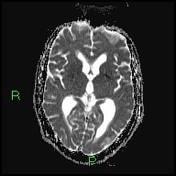
Obstructive hydrocephalus with ventricular enlargement and minor periventricular low density (compatible with transependymal CSF shift).
No supratentorial masses or acute ischemic areas. Right frontal encephalomalacia (presumed prior infarct or trauma). Normal calvarium and skull base.
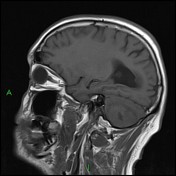
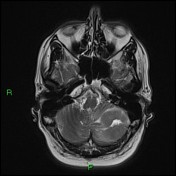
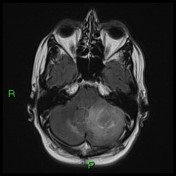
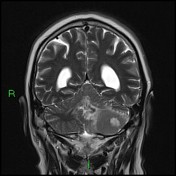
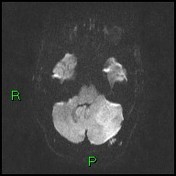

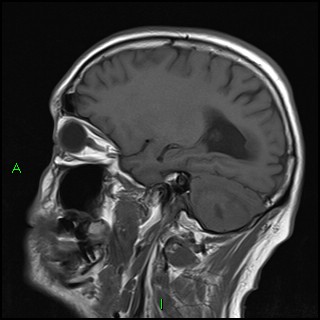
Homogeneously enhancing, solitary, left cerebellar infiltrative mass with mild mass effect and diffusion restriction. Right frontal encephalomalacia. Parenchyma is otherwise normal.
CSF spaces remain prominent, with hydrocephalus. Left occipital bone encephalocele.
Case Discussion
The patient received steroids prior to transfer to the neurosurgical center.
He underwent decompressive resection of the tumor. The post-operative recovery was uneventful.
Pathology returned diffuse large B-cell lymphoma. There was no evidence of other malignancy on investigation and HIV serology was negative.
Chemoradiotherapy was delivered, and follow-up cerebral MR at three months showed no evidence of recurrence.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.