
Presentation
Acute left-sided weakness of the face and upper limb greater than lower limb, sensory inattention, dysarthria. NIHSS 14. Onset 90 minutes earlier.
Patient Data
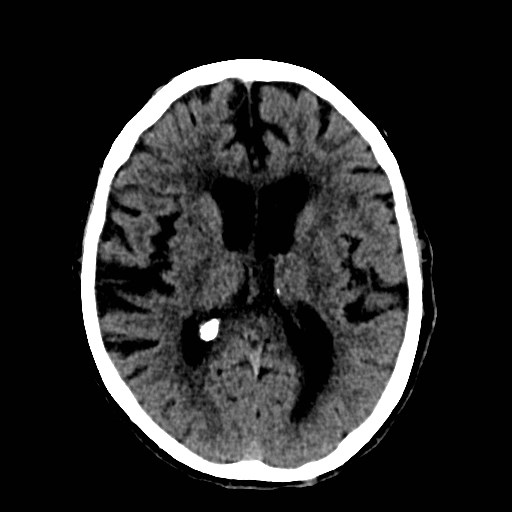
Hyperattentuation of the right MCA M1 segment just distal to its origin from the ICA.
Hypoattenuation of the ipsilateral insular cortex.
Subtle hypoattenuation of the ipsilateral lentiform nucleus.
Background chronic appearing cerebral involution and white matter hypoattenuation.
ASPECTS = 8.
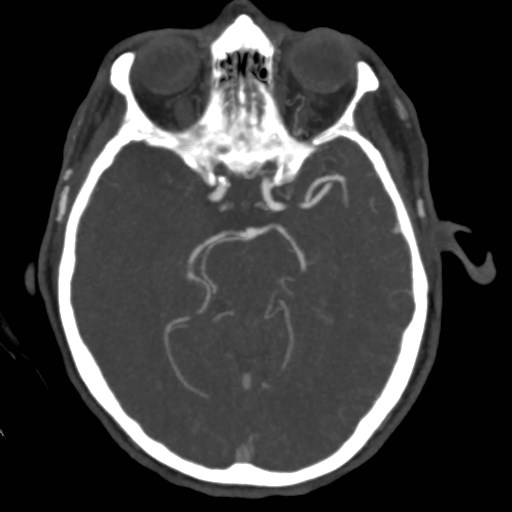
Complete occlusion of the right MCA M1 segment just distal to the ICA bifurcation.
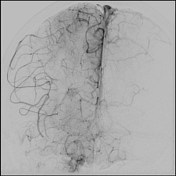


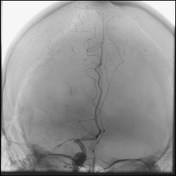
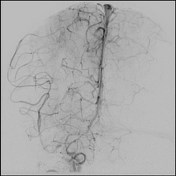

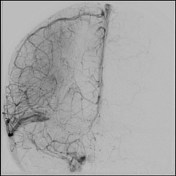
Baseline frontal DSA projection of the right internal carotid artery demonstrating complete occlusion of the proximal right MCA M1 segment and retrograde filling of distal MCA branches from ACA-MCA pial communications. Baseline lateral DSA projection demonstrates retrograde filling of distal MCA branches from ACA-MCA pial communications.
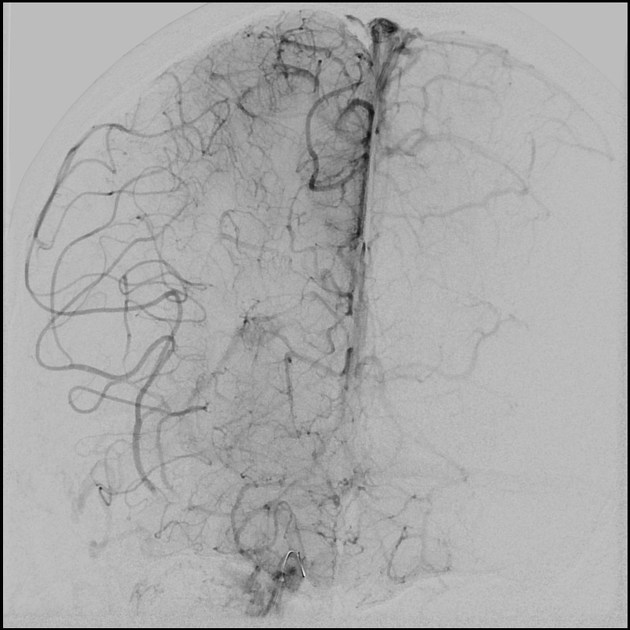
Frontal and lateral right ICA DSA show stent-retriever in situ (Stryker TREVO XP 6 x 25 mm) highlighting the clot and providing "temporary endovascular bypass".
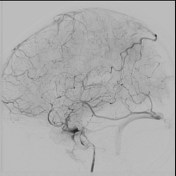
Final DSA following removal of the stent-retriever demonstrating reperfusion of the previously occluded MCA. TICI 2C angiographic result (some underfilling of small distal parietal MCA cortical branches).

The previously demonstrated MCA M1 thrombus has been removed. Expected maturation of previously demonstrated right insular cortex and lentiform nucleus infarction. No new infarction demonstrated. No hemorrhage.
Case Discussion
Good demonstration of hyper-acute non-contrast CT findings in MCA embolic stroke.
DSA images demonstrating the MCA M1 clot and its removal with mechanical thrombectomy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.