
Presentation
Central chest pain, short of breath, abnormal breath sounds at left base. Assess for infection.
Patient Data



Normal heart size and mediastinal contours.
4 x 2 cm lobulated opacity in the left lower zone, with a serpiginous abnormality extending superiorly which may represent a feeding vessel.
Lungs otherwise clear.
Normal heart size.
Recommend urgent contrast CT thorax.


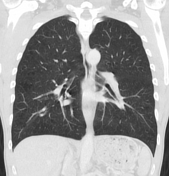
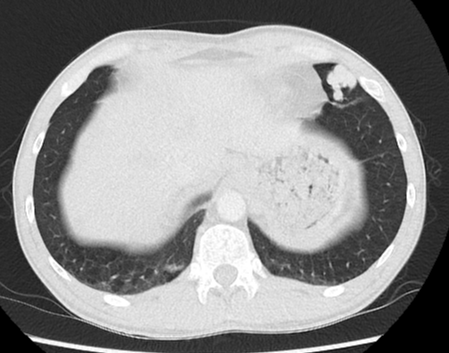
Left lower zone opacity seen on radiograph correlates with an arteriovenous malformation located within the lingula. Single feeding artery arises from the left lingular pulmonary artery and single vein drains into the left superior pulmonary vein. Maximal diameter of feeding artery is approximately 6 mm. Cardiothoracic opinion suggested.
Upper zone predominant predominant emphysema. Lungs otherwise clear. Normal non-dilated heart chambers.
No pleural or pericardial effusion. Mild LAD coronary artery calcification. No aortic valve calcification. No lymphadenopathy. No destructive bony lesions. Vertebral body height and alignment is grossly maintained.
Case Discussion
On plain film imaging this appearance could easily mimic a pulmonary nodule however the large vessel is the clue to the correct diagnosis. Biopsy must be avoided and contrast CT is indicated to identify the number of vessels, additional AVMs any associated vascular pathology such as HHT. Embolization is the preferred treatment and can prevent paradoxical emboli.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.