
Presentation
Known diabetic, hypertensive and thrombocythemia -on warfarin. Presents with dyspnea, difficulty in breathing, right-sided chest pains, unproductive cough, fever, chills, dizziness and palpitations. BP 100/70mmHg, sinus tachycardia 100 bpm, pulse 100, temperature 35.9° C, respiration 30 breaths per minute, SPO2 89%.
Patient Data
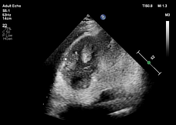

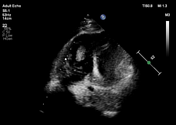


laminated right ventricular apical thrombus measuring 3.0 x 1.6 cm
dilated right cardiac chambers with impaired right ventricular systolic function, tricuspid annular plane systolic excursion (TAPSE) 1.0 mm (normal >17 mm)
severe tricuspid regurgitation with severe pulmonary arterial hypertension, sPAP 63 mmHg




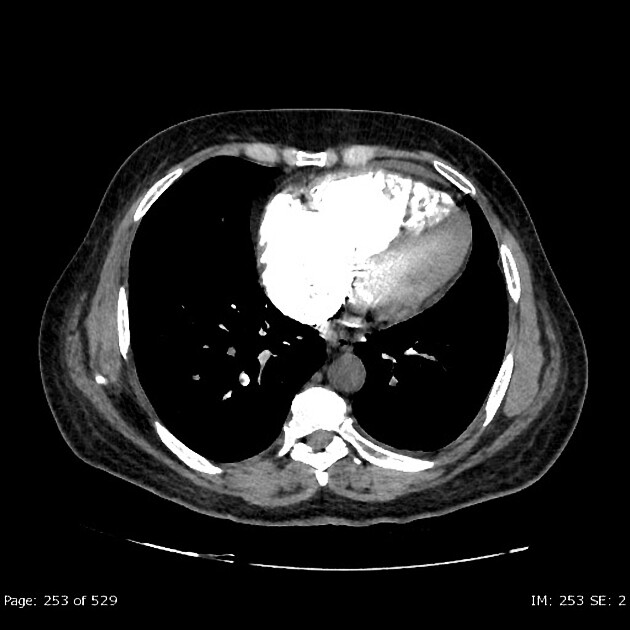
There is an abrupt and complete cutoff in the contrast column in the left main pulmonary artery. Other branches of the left pulmonary artery including lobar, segmental, and sub-segmental arteries to the left lung are not opacified i.e. are blocked. Associated oligemia in the left lung field is demonstrated. Filling defects are seen in the segmental branches of the right pulmonary artery supplying the upper and lower zones.
The right ventricular thrombus is confirmed on CTPA.
The trachea and the esophagus are in normal position. There is no evidence of enlarged lymph nodes. The lung fields are clear and normal. The anterior, middle, and posterior mediastinum are normal.

NB: three ECG leads are noted.
No consolidation or no lung nodules. Normal pleura. Prominence of Right hila due to rotation. No adenopathy. No osseous lesion is noted.
Case Discussion
Right heart thrombus is an uncommon condition found in about 4% of patients with pulmonary emboli 1. Right ventricular thrombus has been found in around 4.5% of patients with pulmonary embolism who underwent echocardiography. The presence of a right ventricular thrombus increases the probability of fatalities and predicts a worse prognosis when compared to pulmonary embolism alone 2.
Echocardiography (transthoracic and transesophageal) is routinely used to identify and evaluate the morphology of the right heart thrombi and aids in treatment decisions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.