
Presentation
Hypertension refractory to antihypertensive medication.
Patient Data

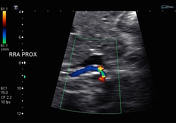

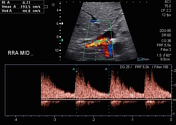

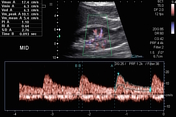
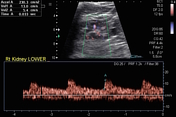
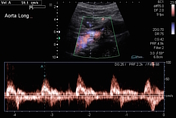
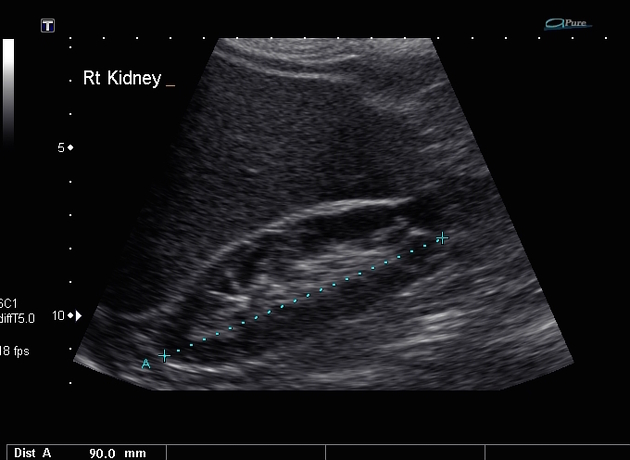
Figure 1. B mode US demonstrates a mildly atrophic right kidney measuring 9 cm in length. Incidental note of a lower pole cortical cyst.
Figure 2. Color aliasing noted at the proximal right renal artery.
Figure 3. Pulsed Doppler sampling reveals elevated peak systolic velocities (PSV) 366 cm/sec at the site of color aliasing.
Figure 4. Turbulent flow is seen downstream in the mid renal artery.
Figure 5-7. There are minimal damping of the segmental internal artery waveform with no significant prolongation of the systolic acceleration time.
Figure 8. The PSV in the juxtarenal abdominal aorta measures 59 cm/sec. The renal artery to abdominal aorta ratio is calculated as 6.2.
Case Discussion
Renal artery stenosis can be encountered in two clinical settings: young patient with fibromuscular dysplasia (FMD) or elderly patient with atherosclerosis. In FMD typically the mid and distal renal artery is affected and more commonly on the right. In contrast the proximal and origin of the renal artery is usually affected in atherosclerosis.
Haemodynamically significant renal artery stenosis can be defined by an elevated PSV at the site of stenosis greater than 180-200 cm/sec. The renal artery PSV to aortic PSV ratio usually exceeds 3.5. Pulsed Doppler can demonstrate aliasing at the site of stenosis with immediate downstream turbulent flow. There can be associated dampening of the arterial waveform in the intrarenal segmental arteries characterized by the parvus-tardus waveform or the internal arterial waveform can be entirely normal.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.