
Presentation
Left flank pain - stones?
Patient Data




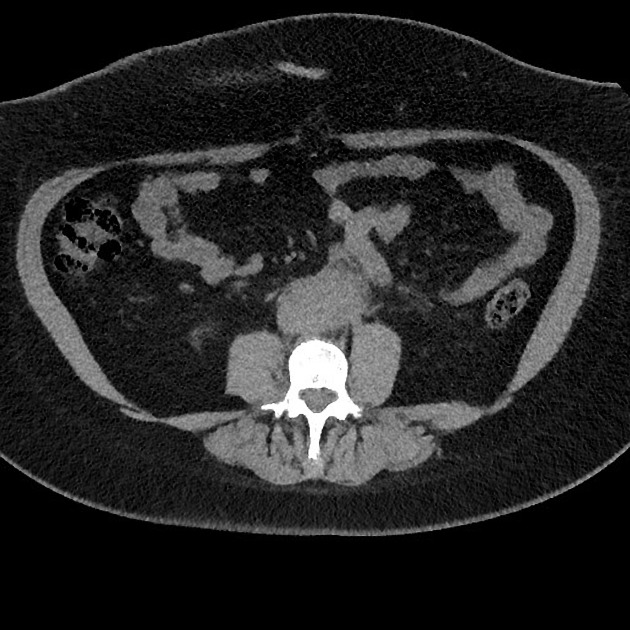
Soft tissue retroperitoneal mass encasing the abdominal aorta and part of the IVC. There is also likely involvement of the left ureter with mild upstream hydroureter and hydronephrosis. Focal calcification within the mass noted.
No renal tract stones. Hepatic steatosis, the abdominal viscera are otherwise unremarkable for this non-contrast scan.



At the subcutaneous planes in the lower anterior abdominal wall, there is a large fluid collection likely representing seroma in this post-operative setting (reasons ignored for the purpose of this case). Minimal surrounding inflammatory stranding.
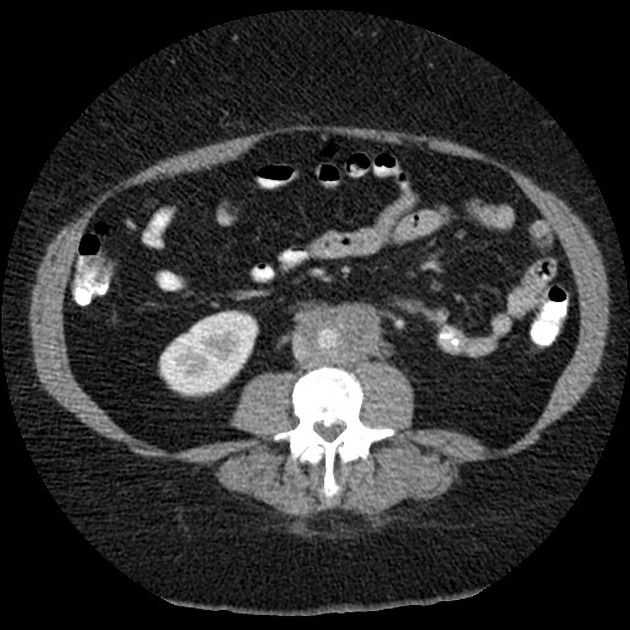
Soft tissue mass surrounding the aorta, extending around the proximal common iliac arteries bilaterally and partially encasing the IVC. Proximal left hydroureter and hydronephrosis. The left kidney is minimally hypo enhancing and demonstrates minimal reduced cortical thickness.
The right kidney is normal in appearance. Although the right ureter is in close proximity to the periaortic soft tissue mass, there is no hydronephrosis or hydroureter.
There is diffuse fatty infiltration of the liver, but no focal lesion. The biliary tree is not dilated. Pancreas and spleen are normal.
Small amount of free fluid in the peritoneal cavity.
No other discrete abnormal lymph nodes.
Case Discussion
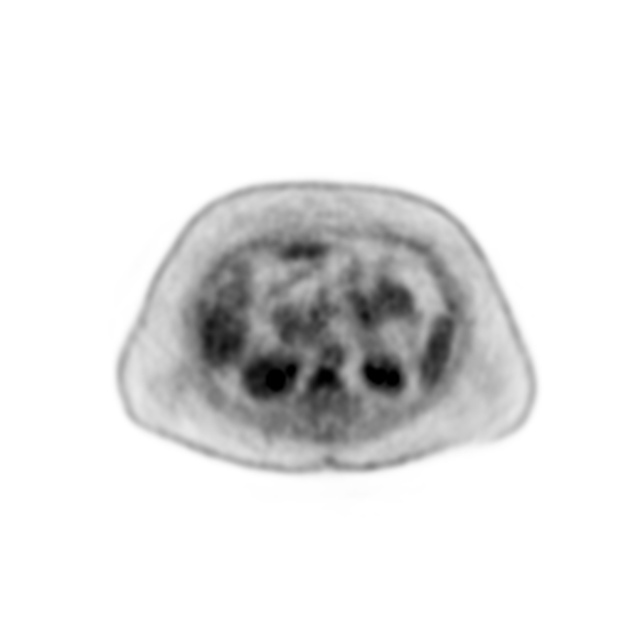
This case illustrates retroperitoneal fibrosis manifesting with partial obstruction of the left renal tract. Retroperitoneal lymphoma is a consideration as a differential, but no discrete lymphadenopathy elsewhere and low metabolic activity makes it unlikely.
A note is made that in between the presentation scan and second CT scan, pelvic surgery was performed for ignored reasons.
Biopsy was performed:
Microscopy: The core biopsies should comprise dense fibrous connective tissue, admixed with moderate numbers of plasma cells and lymphocytes. The tissue extends into fatty tissues. There are no malignant cells.
Conclusion: Features in keeping with retroperitoneal fibrosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.