
Reversible cerebral vasoconstriction syndrome (RCVS) with associated convexity subarachnoid hemorrhage, nimodipine-reversibility
Presentation
Sudden onset of severe headaches and intermittent hyperesthesia of left arm
Patient Data

There is a convexity subarachnoid hemorrhage with high attenuation material within a right frontal sulcus.


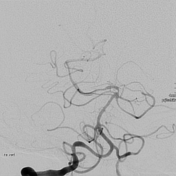

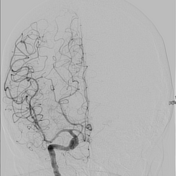

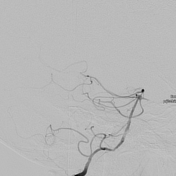
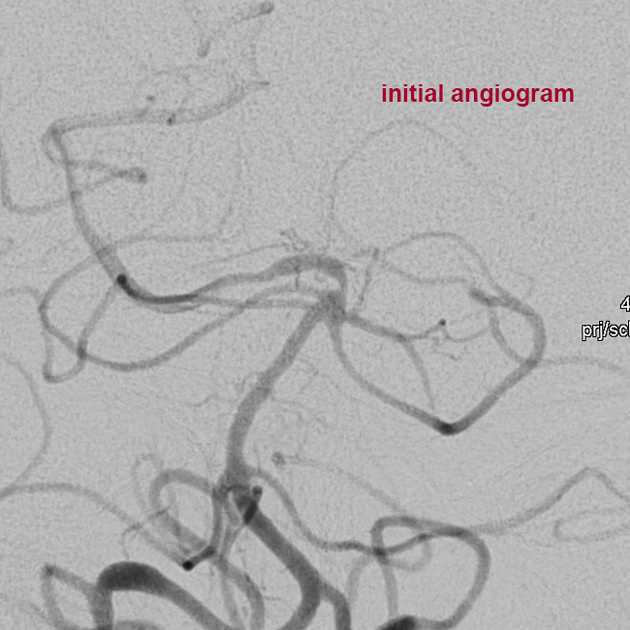
Diagnostic angiogram on day 8 after symptom onset via right transfemoral access (4F).
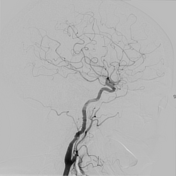
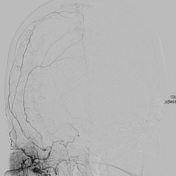
Images of the right ACC, ACI, ACE and bilateral VA are shown.
Right internal carotid artery: Cervical segment shows 'string of beads' sign. Possible FMD (fibromuscular dysplasia).
Right external carotid artery: Diffuse caliber abnormalities.
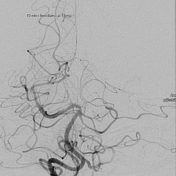
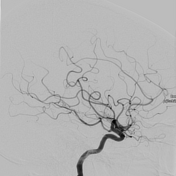
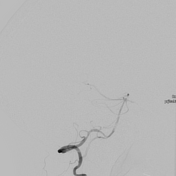
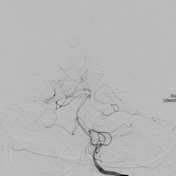
Right vertebral artery: Caliber abnormalities in V3, V4, basilar artery and PCA. The basilar tip appears bigger than the rest of the basilar artery. Left vertebral artery: Smaller than the right VA, V3 caliber irregularity.
Because of diffuse caliber irregularities in MCA and VA territory and recent SAH we suspected RCVS.
After intra-arterial local injection of calcium antagonist nimodipine (1 mg over 10 minutes) reversibility of the caliber changes is demonstrated, normalized diameter of basilar artery.
This raises the probability for RCVS.
No demonstration of aneurysms or vascular malformations as cause for the subarachnoid hemorrhage.
Case Discussion
In a patient with sudden onset of headaches and hypesthesia the same day CT shows a non-traumatic right high frontal subarachnoid hemorrhage (convexity SAH with sulcal localization). CT angiogram shows no aneurysm.
The patient one week later is referred to a neurovascular center. The catheter angiogram 8 days after symptom onset shows no aneurysm or vascular malformations, but diffuse caliber irregularities involving the posterior circulation. This means the vascular changes are seen in a different location than the hemorrhage. Reversibility after intra-arterial calcium antagonist nimodipine (1 mg, 10 mins).
Possible RCVS (reversible cerebral vasoconstriction syndrome) with associated SAH. The time interval since symptom onset (8 days) means SAH-associated cerebral vasospasm is a differential diagnosis, but the localization of vascular abnormalities in the posterior circulation while there is frontal SAH raises suspicion of RCVS. Liquor examination showed WBC, glucose or protein.
No history of drug use, migraine, prior hemorrhage. A follow-up angiogram for the patient is to be scheduled (rule out aneurysm, malformations again). Follow-up liquor examination, follow-up duplex ultrasound scheduled. The patient received nimodipine orally for the following 8 weeks.
Angiogram courtesy of Prof R Chapot and Dr E Celik (Alfried Krupp Krankenhaus Essen, Germany), CT head courtesy of Prof M Dihné (St. Lukas Klinik Solingen, Germany).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.