
Saddle pulmonary embolism with right heart strain and pulmonary infarction
Presentation
Syncope. One week postural dizziness. Troponin positive.
Patient Data


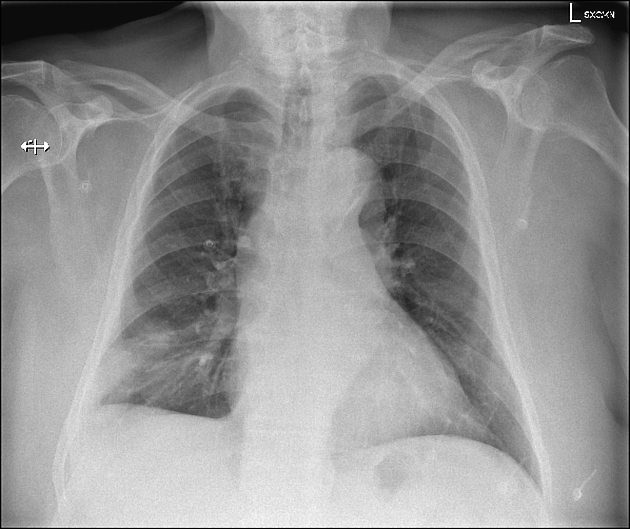
Enlarged cardiac silhouette, CTR of 0.54. Hilar regions are unremarkable. Focal area of air space opacification within the peripheral right lower zone and obscuring the right costophrenic angle. No pneumothorax. No acute bony or soft tissue changes.
DDx for this appearance is infection, hemorrhage or pulmonary infarction due to PE (Hampton's hump).
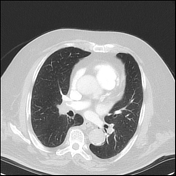

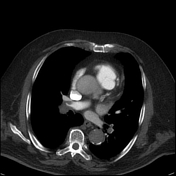


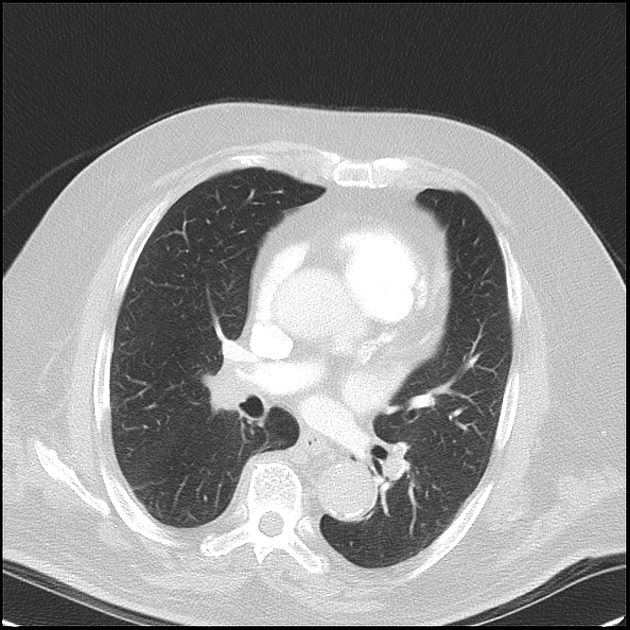
Large saddle embolus extending into the main pulmonary arteries, lobar and segmental arteries bilaterally. The lobar right lower lobe pulmonary artery is completely occluded, and within this distribution peripherally in the right lower lobe are multiple areas of peripheral parenchymal consolidation consistent with pulmonary infarcts (some of these are wedge-shaped). No effusion or pneumothorax. Tracheobronchial tree is patent.
Mildly enlarged pulmonary trunk. Enlargement of the right ventricle, with bowing of the interventricular septum concerning representing right heart strain. Densely calcified left main coronary artery and LAD. Scattered calcification throughout the aorta, and cervical artery origins.
IMPRESSION
Large saddle pulmonary embolism with associated RLL pulmonary infarcts and evidence of right heart strain.
Calcified coronary artery disease, especially of the left main and LAD.
Case Discussion
Nice example of a large burden of PE causing right heart strain and pulmonary infarcts.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.