
Presentation
The patient presented with asymmetric facial deformity and short stature. They sought a consultation due to easy fatigability and shortness of breath.
Patient Data
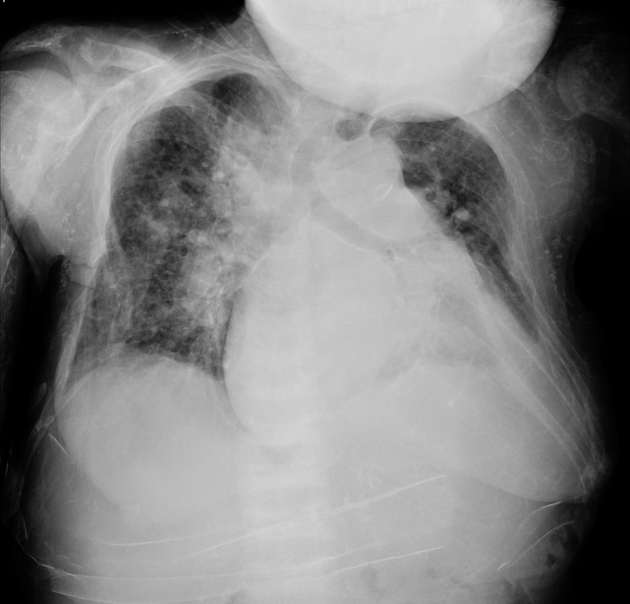
There is an accentuation of the pulmonary vascular markings.
Left-sided pleural effusion is noted.
The heart is enlarged (CTR = 0.6) The aorta is calcified.
There is increased density of the vertebral body end plates (Rugger Jersey spine). Sclerotic changes are seen in the visualized osseous structures. Diffuse subcutaneous calcific densities are seen.
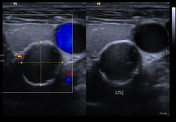

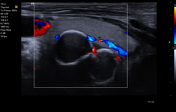
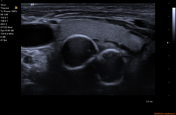
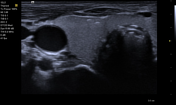
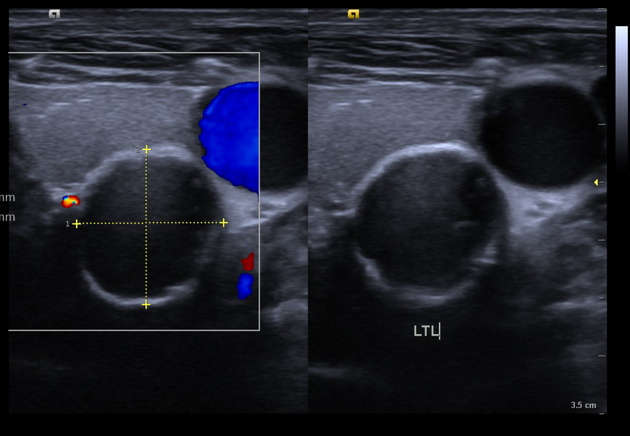
There are two, well-defined, ovoid, hypoechoic lesions with calcific rims posterior to the upper to mid pole of the left thyroid lobe measuring 1.4 x 1.3 cm and 1.3 x 1.0 cm. Likely enlarged parathyroid glands/parathyroid pathology
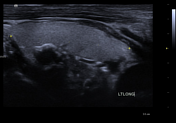
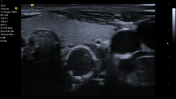
There are two, parenchymal calcifications in the anterior aspect of the lower pole of the right thyroid lobe.
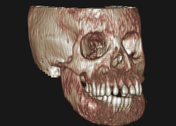

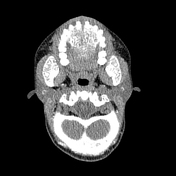


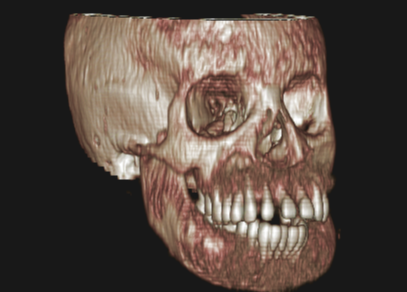
There is bony expansion with heterogeneous bone density ranging from sclerotic to lucent involving the craniofacial bones. The majority of affected bones demonstrate a ground-glass appearance. Extensive bony expansion is noted involving the entire mandible and maxilla.
Case Discussion
This uncommon bone condition is marked by secondary hyperparathyroidism in patients suffering from chronic kidney failure. It is brought on by inadequate management during the initial stages of the disease, leading to phosphorus retention, vitamin D deficiency, and disrupted calcium-phosphorus metabolism, all of which raise parathyroid hormone levels. Patients may have hearing loss, mental issues, dental anomalies, significant alterations to the skull and jaws, severe changes to other skeletal malformations, and short height.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.