
Presentation
Patient noticed nodulations in the neck and experienced shortness of breath.
Patient Data


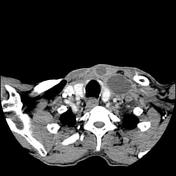


Computed tomography of the neck and thorax show necrotic cervical lymph node enlargement, calcified mediastinal and hilar lymph nodes, multiple pulmonary nodules, cavitations in the right lung, fibrosis with architectural distortion in both lungs, and multiple splenic calcifications.
Case Discussion
Pulmonary tuberculosis is reported to be higher in those patients with silicosis. The imaging appearances of the lungs, with all the architectural distortion and fibrosis, make it difficult to asses for tuberculosis, with the clinical picture being essential to raise suspicion for the associated infection. In this case, the multiple necrotic lymph nodes in the neck are highly suggestive of TB, and the cavitation in a conglomerate fibrotic mass points also for possible lung involvement.
The multiple calcifications involving the imaged spleen can be attributed both to tuberculosis or silicosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.