
Presentation
Abdominal pain.
Patient Data
Presentation radiograph



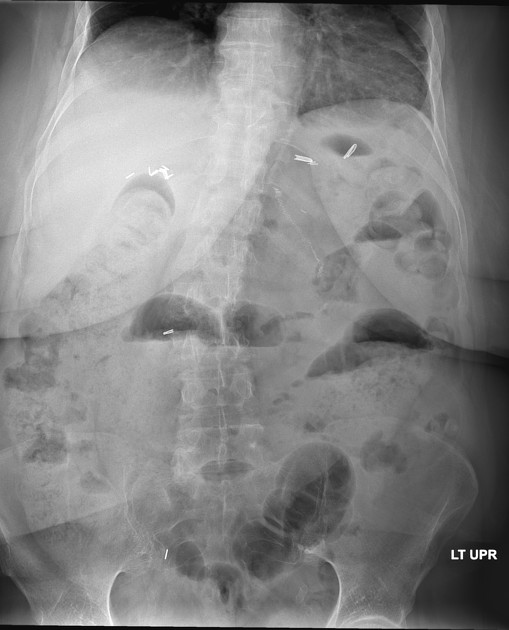
Several surgical clips. Medium to large amount of colonic stool. Two air-fluid levels in the mid abdomen on upright.
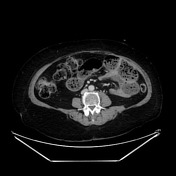




Fluid filled distal esophagus. Antecolic roux-en-y gastric bypass which is dilated and fecalized proximally leading into an abrupt, angulated midline transition point before the JJ anastamosis. The distal small bowel is decompressed.

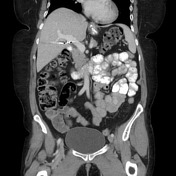


Antecolic roux-en-y gastric bypass with normal caliber bowel.
Case Discussion
The fecalized segment of the proximal small bowel leads to an abrupt transition in the midline characterized by angulation and distal decompression leading into the JJ anastomosis. It would be reasonable to consider an internal hernia in this case, however, the distal small bowel remains decompressed and does not exit any hernia defect.
Operative note excerpt: "We proceeded to takedown noted adhesive disease along the abdominal wall with energy device. We inspected the abdomen running the bowel proximally back from the terminal ileum noting an area of transition of decompressed bowel to dilated bowel. This area appeared densely adhered to the retroperitoneum in addition to the surrounding mesentery..." This surgery was ultimately converted to open resection due to difficulty with freeing the small bowel from the surrounding adhesions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.