
Presentation
Distended abdomen. Passing flatus. Raised white cell count.
Patient Data
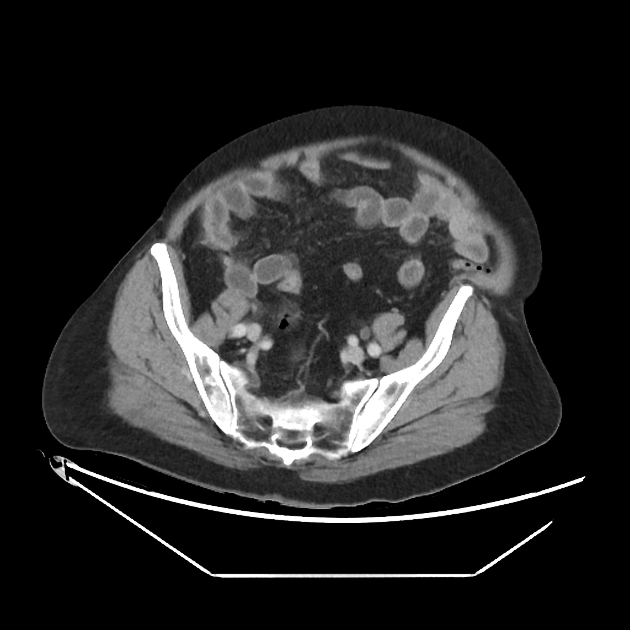
CT study reveals small bowel distension, with no definite transition point.
However, there is subtle fat stranding in the right iliac fossa and an inflamed appendix.
Incidental non-obstructed indirect hernia in the left iliac fossa, containing large bowel.
Oral contrast follow-through



The contrast follow-through revealed there was no complete obstruction, with oral contrast seen in the rectum
Case Discussion
The patient presented with abdominal pain and vomiting. On examination, there was considerable abdominal distension and additionally raised inflammatory markers.
CT revealed small bowel distension with no definite transition point. However, there is subtle fat stranding in the right iliac fossa and an inflamed appendix.
This case highlights how patients with acute intra-abdominal infection can present with obstructive symptoms, when in fact, there is not complete obstruction and this is a case of small bowel pseudo-obstruction secondary to appendicitis.
The appendicitis was managed successfully and conservatively with antibiotics.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.