
Presentation
Shortness of breath.
Patient Data


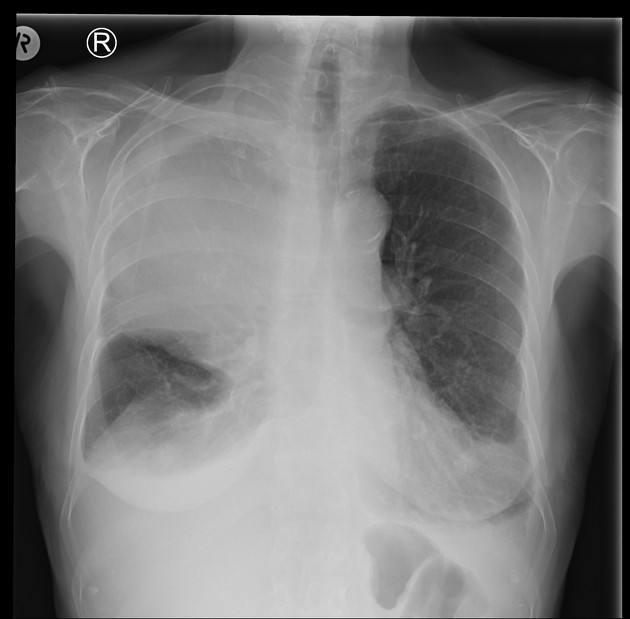
There is extensive white-out involving the right upper lobe anterior aspects. It is uncertain if this represents a pleural based mass pushing the lungs posteriorly or a parenchymal mass. Small to moderate volume of pleural effusion on the right. Mediastinal contours are unremarkable, with negative silhouette sign with the withe-ou area. No destructive bone lesions.
Further CT chest advised.


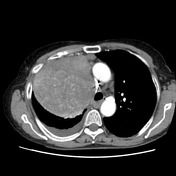




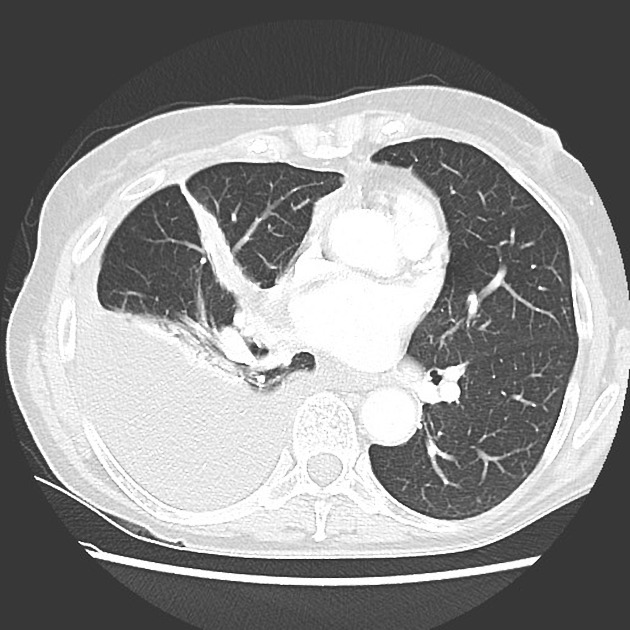
Large heterogeneous mass in the superior right hemithorax displacing the mediastinum to the left and partially effacing the superior vena cava. The mass extends posteriorly into the right paratracheal space with no intervening fat plane. Retrosternal soft tissue nodule in the anterior mediastinum appears to be continuous with the mass, although may represent a lymph node. The lesion appears to be pleural based; a mediastinal mass is felt unlikely.
No erosion or periosteal reaction of the adjacent ribs. Associated large low-density pleural effusion. Partial collapse of the right lower lobe and atelectasis in the middle and upper lobes. The left hemithorax is clear.
Multinodular thyroid goiter.
Calcified granuloma in the spleen.
Multiple vertebral body hemangiomas.
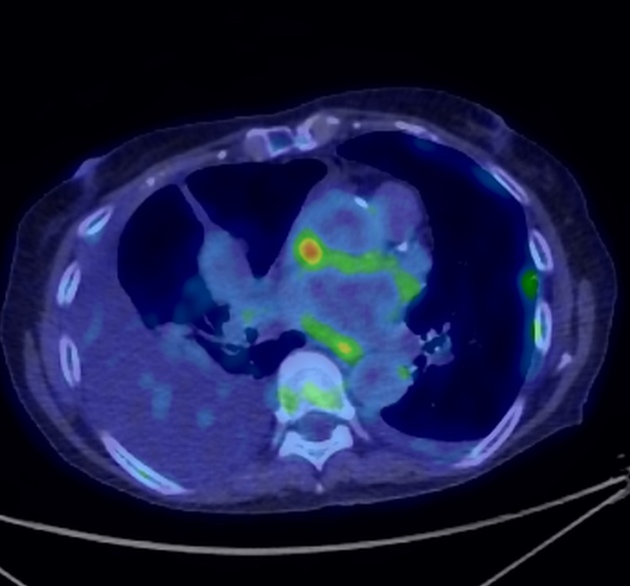
There is only minimal FDG activity distributed heterogeneously in the very large mass centered in the superior right hemithorax. There is associated partial collapse of the right upper, middle and lower lobes. These findings suggest a low-grade neoplastic process.
There is minimal nonspecific FDG activity in the large right pleural effusion, small left pleural effusion, and along the left lateral pleural margin.
Minimal FDG activity in the left lower paratracheal mediastinal nodes is non-specific.
Intense FDG activity in the interatrial septum is without structural CT correlate and explainable by a benign cause (eg lipomatous hypertrophy of the interatrial septum).
No increased FDG activity is demonstrated in the splenic granuloma or in the thoracolumbar vertebral body hemangiomas. No increased FDG activity is demonstrated in the multinodular goiter.
No further abnormal foci of increased FDG activity are demonstrated in the neck, chest, abdomen or pelvis to suggest FDG avid malignant disease.
Macroscopy: Sectioning shows homogenous firm grey tissue attached to a thin strip of the lung parenchyma, 1 mm in thickness. The stapled resection margin is inked black, with the remainder inked blue. "Right chest wall mass". An excision of lobulated cream-colored/pink tissue. No normal lung tissue is identified, nor is any obvious resection margin. Scant adipose tissue with attached. Sectioning shows lobulated whorled cream-colored lesional tissue with prominent fibrosis. No necrosis, hemorrhage or calcification is present. The external surface is inked blue.
Microscopy: The sections show a nodular lesion arising at the visceral pleural surface, comprised of haphazard arrays of spindled cells with intervening thick ropey collagen, and scattered ectatic, irregularly branched and thin-walled vessels. The spindled cells have tapered nuclei, evenly distributed nuclear chromatin and occasional small nucleoli, and show only minimal variation in size and shape. Scattered chronic inflammatory cells are seen. Mitotic figures are rare. The lesion is present at the pleural surface and focally abuts the stapled resection margin. A small amount of uninvolved perilesional lung parenchyma present near the stapled resection margin shows type 2 pneumocyte hyperplasia.
The sections show a tumor with a multinodular architecture, traversed by fibrous connective tissue bands of variable width. The tumor is comprised of haphazard arrays of spindled cells with intervening thick ropey collagen, with scattered ectatic and irregularly branched, thin-walled vessels throughout. The spindled cells are plump, blunt-ended, closely packed and exhibit moderate variation in nuclear size. Chromatin is fine and evenly distributed and cytoplasm small to moderate in amount and showing variable eosinophilia. Whilst the bulk of the tumor is highly cellular, areas of hypocellularity associated with myxoid stromal change are present. Focal necrosis is identified. Mitoses are numerous, numbering up to 8 within 2 square millimeters). Evidence of dedifferentiation is not observed. Angiolymphatic invasion is not identified. Tumor extends to the resection margins of the specimen. A small amount of alveolates lung parenchyma is noted and, in this section, the appears to arise at the visceral pleural surface. A small amount of uninvolved mature adipose tissue is noted.
Tumor cells show nuclear immunoreactivity with antibodies against STAT6, cytoplasmic immunoreactivity with antibodies against Bcl-2, CD99 and beta-catenin, and patchy cytoplasmic immunoreactivity with antibodies against CD34.
Immunohistochemistry with antibodies against pan-cytokeratins, ALK1, CK5/6, desmin, SMA, caldesmon, podoplanin, S100, calretinin, WT1, EMA and p53 is negative.
Conclusion: Solitary fibrous tumor.
Case Discussion
Solitary fibrous tumor of the pleura usually presents in elderly patients as large well-defined solid pleural based masses. heterogeneous enhancement seen in these tumors is due to myxoid degeneration. Metastasis, pleural lymphoma, and mesothelioma, although possible differentials are considered unlikely given the size and low-avidity on PET.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.