
Presentation
Low back pain
Patient Data
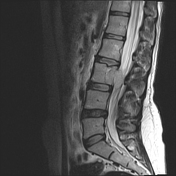


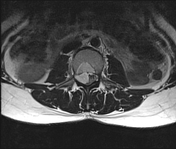


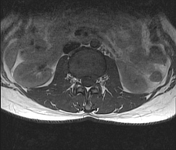
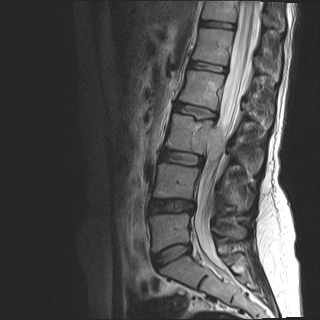
There is a mass at posterior aspect of L3 vertebral body that shows high T2 signal intensity and enhances.
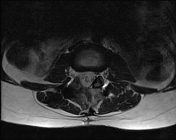
Associated epidural component which is almost the same size as the bony component, compresses and displaces the thecal sac. CSF is obliterated at this level.
There is extension to right neuroforamen.
The patient proceeded to biopsy, which proved to be "chordoma".
Subsequently, laminectomy and debulking of the epidural component were done.



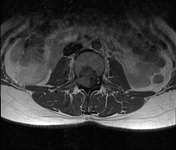
The postoperative images show that the epidural component has been removed, eliminating the compression effect on the thecal sac, however the neuroforamenal component still persists probably due to difficult access and proximity to the nerve roots.
Histology:
Gross: Received specimen is multiple pieces of gray tissue with semi-firm consistency m: 3*2 cm totally.
Microscopic examination: Sections show neoplastic proliferation of mildly atypical cells with abundant clear to eosinophilic cytoplasm arranged in nests and cords and embedded in myxoid stroma.
Final diagnosis: Lumbar spinal lesion resection:
Chordoma
IHC results:
CK: Positive
EMA: Positive
S100: Negative
GFAP: Negative
Case Discussion
Chordomas are slow-growing but locally invasive and highly recurrent tumors. Amongst primary spinal malignancies, they are second only to lymphoproliferative diseases. The vertebral body is mostly involved in spinal chordomas. Metastasis and plasmacytoma are among the differential diagnosis.
After pathological confirmation, patient went on to have resection and radiotherapy as needed.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.