
Synchronous acute appendicitis and epiploic appendagitis of the appendix
Presentation
Slight discomfort in right lower quadrant for 1 week. Acutely aggravated at day of presentation to emergency service together with chills and fever. Nausea but no vomiting. Muscular defense in right lower quadrant, but no deep tenderness at McBurney´s point. Pyrexia, elevated leukocyte count and C-reactive protein.
Patient Data


There is a contrast-enhancing fluid-filled dilated blind-ending tubular structure in the right lower quadrant with an outer diameter of 12 mm. In addition to the haziness of the mesoappendix, focal edematous thickening of the cecal pole and focal peritoneal thickening in the right iliac fossa, ovoid contrast-enhancing lymph nodes in the ileocecal station without lymphadenopathy after size criteria are also noted. While a small amount of free intraperitoneal fluid is seen in the pouch of Douglas, there are no organized fluid collections.
The antimesenteric site of the tip of the appendix houses a 2 cm ovoid sharply demarcated fat-containing lesion which is intervened by branching thin tubular hyperdensities.
Incidental note is made of a small hiatal hernia, sliding type, a splenule at the upper lateral pole of the spleen, colonic diverticulosis and a vesicourachal diverticulum without evidence of infection. Degenerative spine disease with a single-level posterior disc calcification (L5/S1) without herniation is also noted.
The remainder of the study is within normal limits.
Impression
CT findings are strongly suggestive of acute appendicitis.
Synchronous epiploic appendagitis of the appendix is likely.
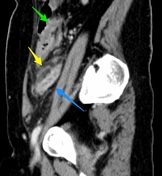


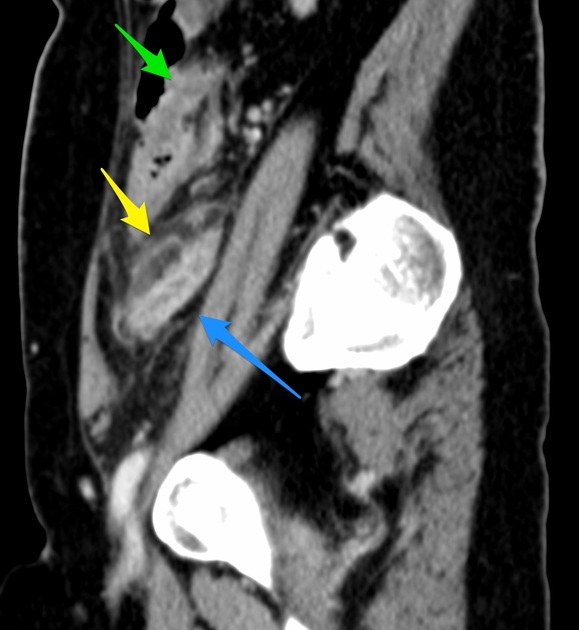
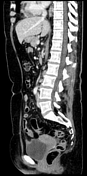
Sagittal CT MPR at the level of the right psoas muscle depicts a fluid-filled, contrast-enhancing dilated structure (blue arrow) with haziness in the mesoappendix (yellow arrow) and edematous thickening of the cecal pole (green arrow).
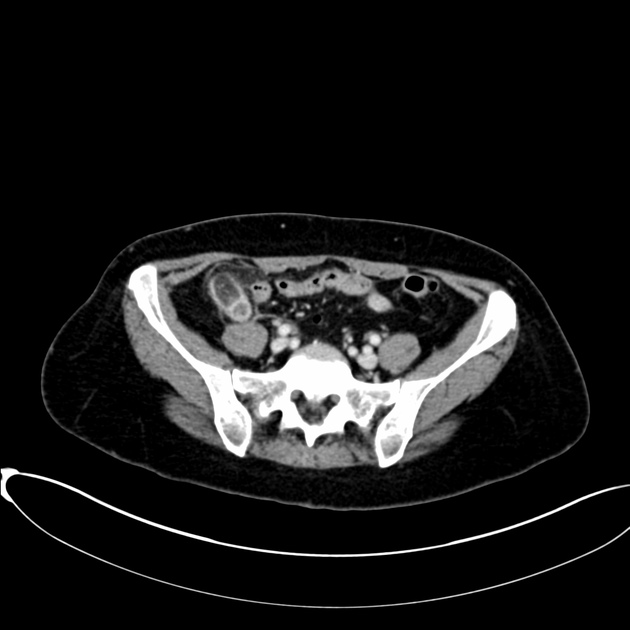
Axial CT MPR at the level of the iliac crests again shows fluid-filled, dilated vermiform appendix with contrast-enhancing mucosa (blue arrow). A well-marginated, ovoid fat-containing mass off the tip of the appendix with central dotted hyper densities (orange arrow) is also appreciated.
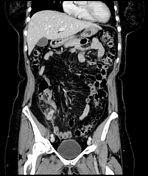
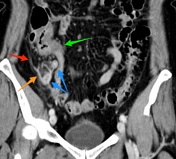
Coronal CT MPR at the level of the great vessels shows contrast-enhancing, round to ovoid lymph nodes in the ileocecal station (yellow arrows) without lymphadenopathy after size criteria. Note focal peritoneal thickening in the right iliac fossa (cinnabar red arrow).
Coronal CT MPR at the level of the symphysis depicts mucosal enhancement of the fluid-filled, dilated vermiform appendix (blue arrows) together with edematous thickening of the cecal pole (green arrow). Focal peritoneal thickening (red arrow) is noted as well as a well-demarcated fat-containing ovoid mass off the tip of the appendix at the antimesenteric site (orange arrow).
The patient was taken to the surgical theater and laparoscopic appendectomy was performed.
The thickened, non-perforated vermiform appendix with extensive omental adhesions and an indurated tip was removed without complications. The patient made an uneventful recovery and was discharged on the first postoperative day.
Pathology report
Macroscopic description:
Received an 8 cm long tubular structure, fibrin-covered and hemorrhagic, with an outer diameter varying from 0,5 cm to 1,1 cm. No apparent perforation on cut surfaces. The cut surface of the thickened tip is dominated by fat.
Microscopic description:
Sections from apex to base of appendix show mucosal ulcerations of varying size and up to intensive neutrophil invasion in all layers with impending perforation but conserved muscular layer in all sections. The outer surface of the appendix is covered by a thin layer of fibrin containing polymorphic granulocytes. Sections from indurated area at the apex show a mixture of normal adipocytes interspersed by hemorrhage, anucleated adipocytes and foamy histiocytes. No malignancy.
Conclusion
Acute appendicitis with a gangrenous epiploic appendage.
Case Discussion
While acute appendicitis is a common cause of acute abdomen, epiploic appendagitis of the vermiform appendix is rare. Apart from the location, they do not have much in common; in fact, both prognosis and treatment options vary grossly. The former is commonly addressed by emergent surgical consultation and appendectomy, while the latter very often being self-limiting and usually treated by pain medication.
The clinical presentation and hospital course of this 50ish female are suggestive of oligosymptomatic epiploic appendagitis of the vermiform appendix a week prior to acute onset of acute appendicitis at the day of presentation to the ER. However, acute appendicitis with insidious onset and secondary torsion of the epiploic appendage cannot be ruled out.
Whichever way, this case highlights the high accuracy of CT in the diagnosis of acute abdomen, especially with the use of multidetector CT scanners and multiplanar reconstructions, as actually both entities were correctly predicted allowing for both timely and curative treatment.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.