
Presentation
Fall. Parapelgia.
Patient Data





Normal craniocervical junction.
C5/6- Large disc prolapse at C5/C6. This combined with posterior longitudinal ligament calcification is severely compressing and distorting the cord, with both high signal and expansion of the cord at the C5/C6 level, consistent with the cord compression with cord edema opposite the C5 and C6 vertebral bodies. Minimal calcification within the prolapsed disc suggesting a large component of this is acute.
Bilateral foraminal stenosis also at C5/C6 due to neurocentral osteophytosis.
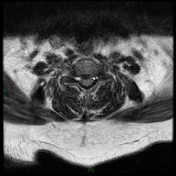
Small left paracentral disc osteophyte complex at T6-T7. No cord compression or nerve root impingement.
Left paracentral disc osteophyte complex at T10/T11 contacting the ventral aspect of the cord with mild exit foraminal narrowing. No nerve root impingement.
Diffuse disc osteophyte complex T11/T12 with left-sided asymmetry, contacting the ventral aspect of the cord. No cord or nerve root impingement.
Case Discussion
Traumatic C5/C6 cord compression due to an acute disc prolapse on the background of chronic disc disease.
CT was undertaken prior to the MRI on which no bony injury was identified.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.