
Presentation
Prostate cancer (Gleason 10) diagnosed two years earlier, treated with radical prostatectomy with pelvic lymphadenectomy and targeted radiotherapy. Recent biochemical recurrence, suspected vertebral metastasis on a subsequent PET-CT. No back pain.
Patient Data


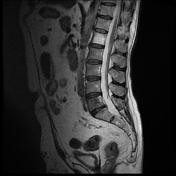
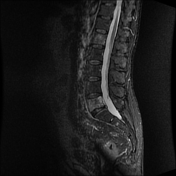
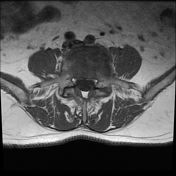
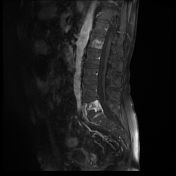
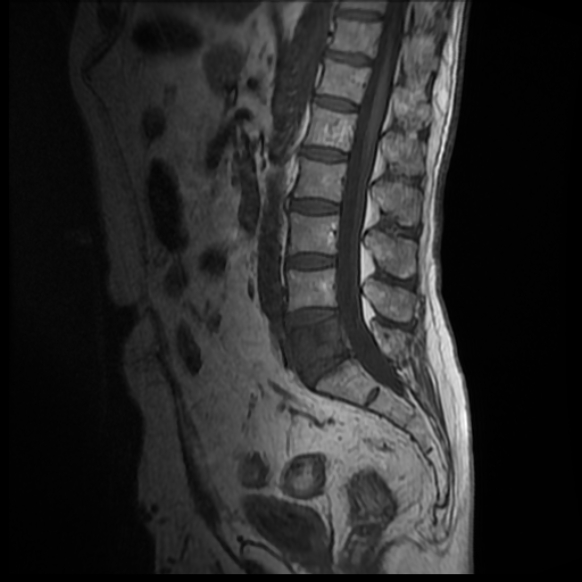
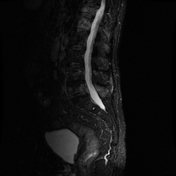
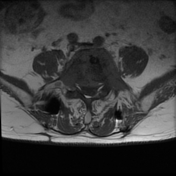
Complete pathological replacement of the L5 vertebral body, without extension to the pedicles. There is a small fracture/Schmorl node of the L5 superior vertebral endplate, but the vertebral body height is maintained. The overall appearance is in keeping with an L5 vertebral metastasis in the setting of prostate cancer.
Apart from that, no suspicious lesions within the visible bony structures.
A large vertebral hemangioma of the L1 vertebral body is visible, with a typical polka-dot appearance. A second, smaller hemangioma can be seen in the left L1 pedicle.
The patient underwent L5 vertebroplasty and L4-S1 transpedicular stabilization.
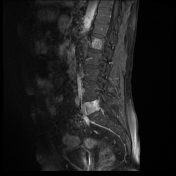
Interval L5 vertebroplasty and L4-S1 transpedicular stabilization.
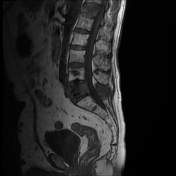
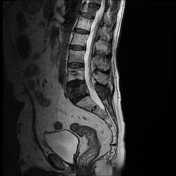
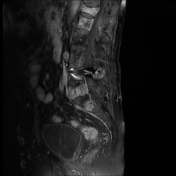
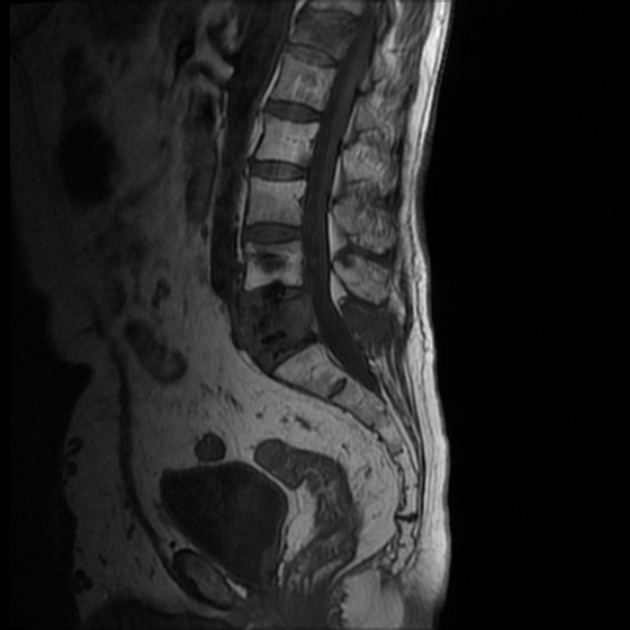
Multiple new metastatic lesions are visible, scattered in all visualized vertebrae, the sacrum and both iliac bones. Some of the lesions involve the vertebral pedicles and posterior elements. There is associated synovitis in the right T12-L1 intervertebral joint.
The T12 vertebral body is pathologically replaced, with a compression fracture, moderate/severe height loss and mild retropulsion of the superior posterior cortex into the ventral epidural space, but with no significant thecal sac compression and no spinal cord compression.
The L5 vertebral body infiltration is more extensive than in the previous study, involving also both vertebral pedicles and the posterior elements. There is mild bulging of the posterior cortex into the ventral epidural space. Post-vertebroplasty cement is visible inside the L5 vertebral body and L4-L5 disc.
Case Discussion
The appearance of the visualized lesions in connection with the clinical history make this a straightforward diagnosis. The patient reported no history of fall or any trauma to the lumbar region between the two examinations, so a benign etiology of T12 fracture is highly unlikely, even though there is a posterior cortex retropulsion rather than bulging.
Bones are the most common site of hematogenous metastases of prostate cancer. The spread may be very rapid, as in this case, where it took only eight months since the PET-CT and the initial MRI study to progress into multiple visible metastatic lesions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.