
Acetabular labral tear, as the name implies, is a tear involving the acetabular labrum of the hip. It is defined as a defect in the labral surface, intralabral surface or chondrolabral junction 10.
With the increasing use of hip arthroscopy in orthopaedic surgery since the 1970s, pathologies of the acetabular labrum as a possible cause of chronic hip and groin pain have become more familiar to a wider medical audience.
On this page:
Epidemiology
Acetabular labral tears are not infrequent. They are found in 55% arthroscopies for intractable hip pain 1.
Associations
femoroacetabular impingement and related structural osseous abnormalities
capsular laxity
cartilage damage
Clinical presentation
Often labral tears cause no symptoms.
If symptomatic, they are associated with:
pain on weight-bearing, flexion and internal rotation
microinstability, painful audible clicking, transient locking, giving way of the hip
mismatch between clinical symptoms and radiographic findings, which often leads to delayed diagnosis
long-standing labral tears contribute to premature osteoarthritis 1,2
Pathology
Major trauma (e.g. hip dislocation) may cause a labral tear. However, there is no history of previous trauma in most cases. Structural osseous abnormalities are often found 3-4. Patients with osteoarthritis often have degenerative labral tears.
Most of the symptomatic tears are located in the anterosuperior quadrant 10.
Radiographic features
Plain radiograph / CT
normal appearance in most cases
structural skeletal abnormalities
osteoarthritis (advanced cases)
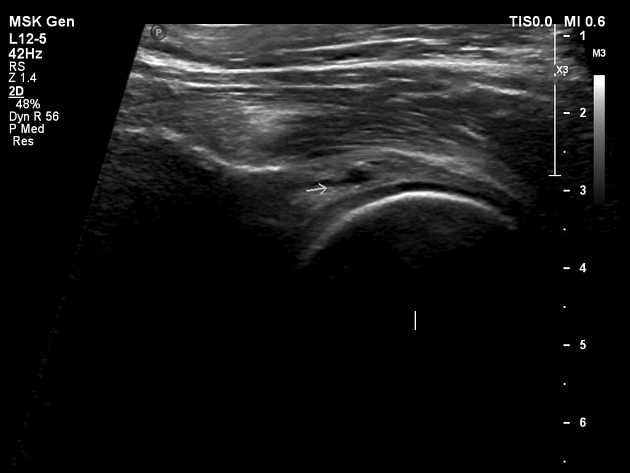
Ultrasound
Labral tears may manifest as abnormal labral morphology, hypoechoic cleft and/or labral detachment from the acetabular rim. Paralabral cysts may also be visible 7.
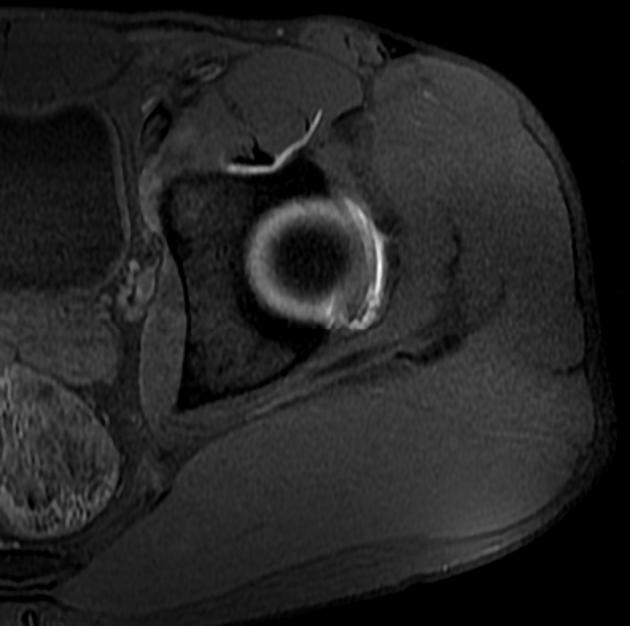
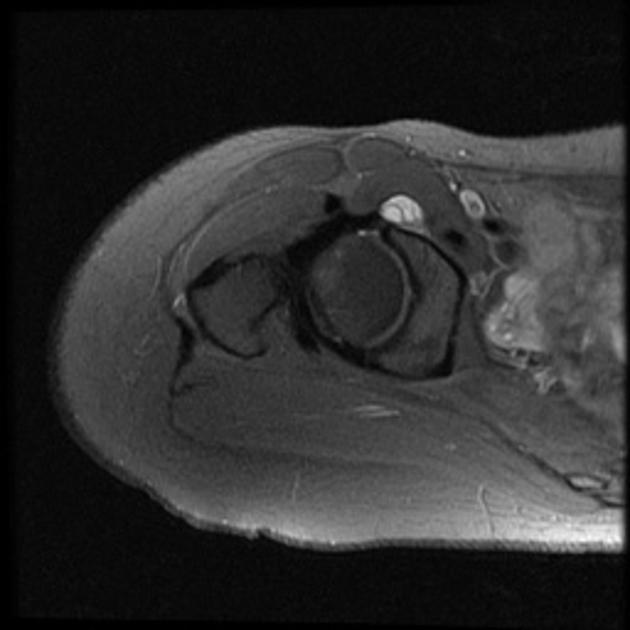
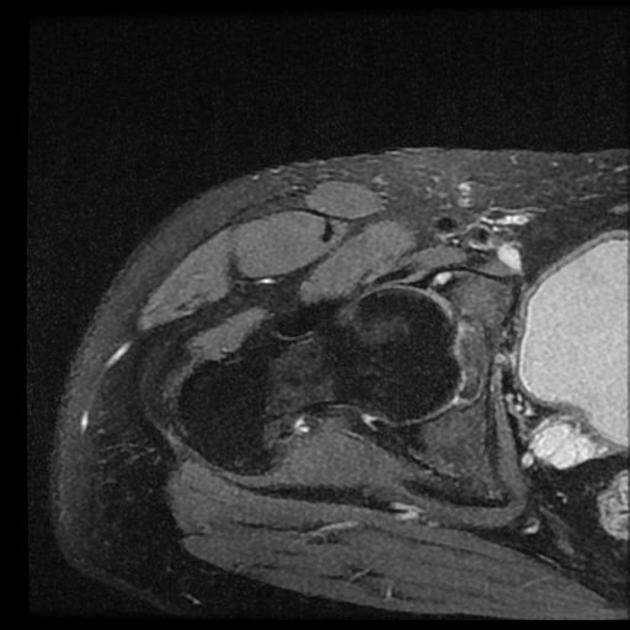
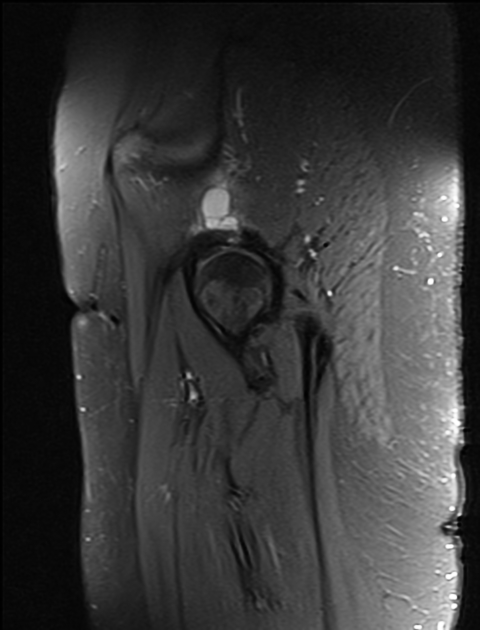
MRI
labrum integrity can be assessed only in the presence of joint effusions (in which case fluid is seen penetrating through labral contour or chondrolabral junction)
additional findings may be present, such as displaced labrum, chondral injury, paralabral cyst or stripping of the capsule
intrasubstance high T1 or PD signal is not considered as pathologic
high T2 signal may be interpreted as mucoid or cystic degeneration
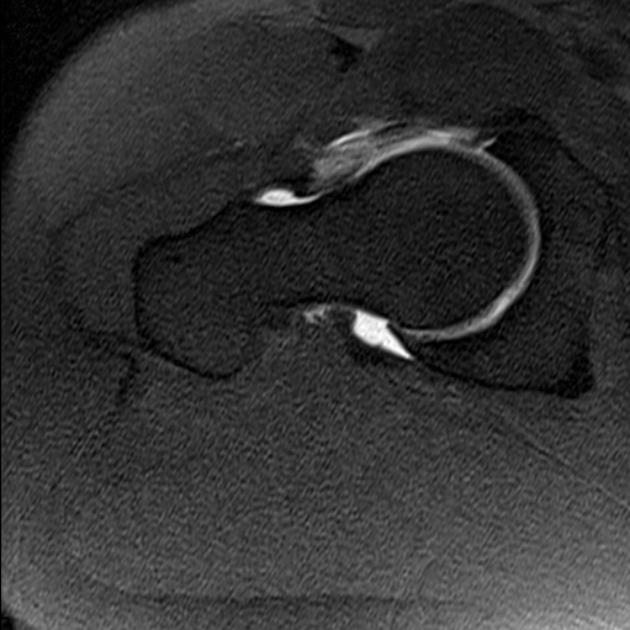
Direct MR arthrography
most accurate imaging study (91% vs 36% on native MRI)
minimally invasive compared with arthroscopy
highly diluted intra-articular Gd-injection (0.0025 mmol/ml) with joint distension (10-20 ml) allows optimal assessment of the labrum on T1 fatsat sequences, and allows to differentiate between labral tears and intrasubstance tears
Normal findings
triangular cross-section
rounded/flattened labral cross-section
perilabral cleft
insertional cleft on the transverse ligament
communicating iliopsoas bursa (15%)
Controversial findings
absent antero-superior labrum
sublabral sulcus
Pathologic findings
-
labral tears (marked by intrasubstance contrast entry)
longitudinal
bucket handle
flap
radial
cleavage
labral detachment
cartilage delamination
loose bodies 1
Radiology report
The labral tears are reported using quadrants or a clock-face.
History and etymology
It is thought have been first described by Petereson in 1957 12.
Treatment and prognosis
Conservative management consists of activity modification, non-steroidal anti-inflammatory drugs, physical therapy and intra-articular injections 9. Acetabular labral tears are the main indication for hip arthroscopy which is the gold standard 9,10. Partial labrectomy and labral repair are the current surgical options.
Preliminary scientific data suggest that labral repairs can heal and patients can expect both symptomatic and functional improvement. However, valid prospective studies are needed to determine the long-term outcome of labral repair 5,6.
Differential diagnosis
On arthrography for small clefts consider:
labral sulci (developmental normal variant): sulci have smooth labral edges, whereas labral tears tend to have irregular edges




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.